SHOULDER
Giasna Giokits (Jasna Jokic)
Pathology of the tendon of the Long Head of the Biceps muscle (LHB)
Tenosynovitis of the Long Head of the Biceps muscle
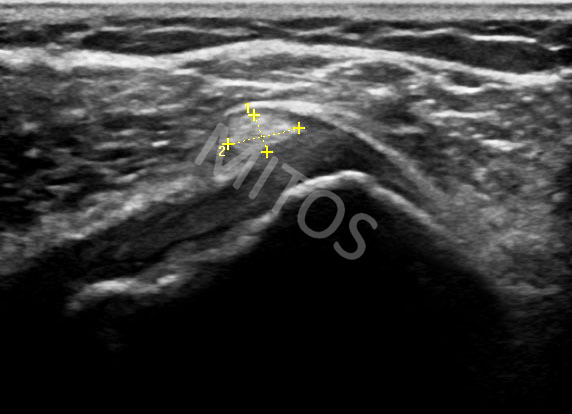
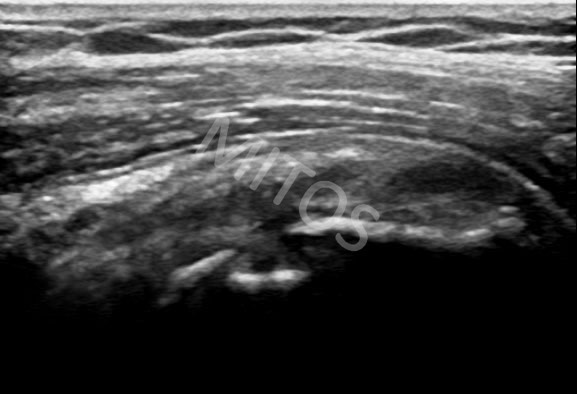
In the case of tenosynovitis, by means of ultrasonographic imaging, a fluid collection is detected within the tendon sheath in a view of an anechoic halo, (figure 1). This fluid collection is often accompanied by pathologic appearance of the tendon itself. The LHB is visualized as an enlarged and of mixed echogenicity structure, and should be evaluated in both sonographic planes.
{kind=link}
Subluxation / Dislocation of the Long Head of the Biceps muscle (LHB)
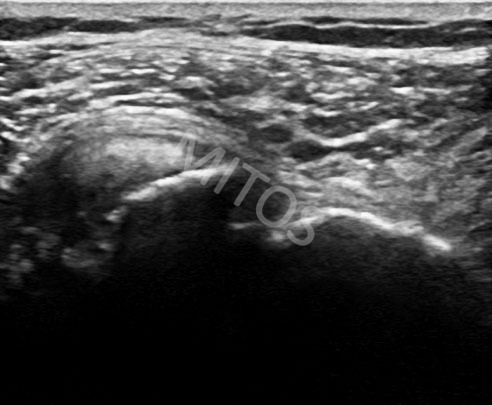
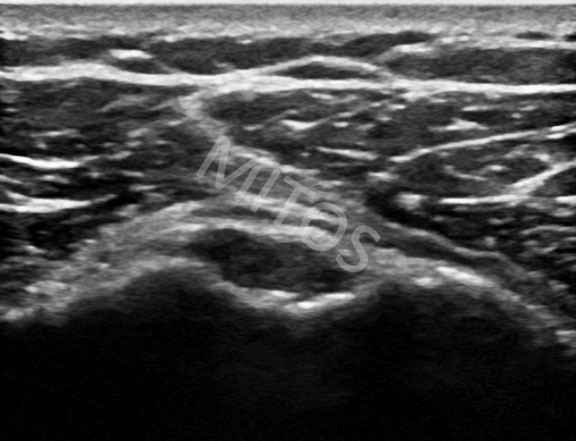
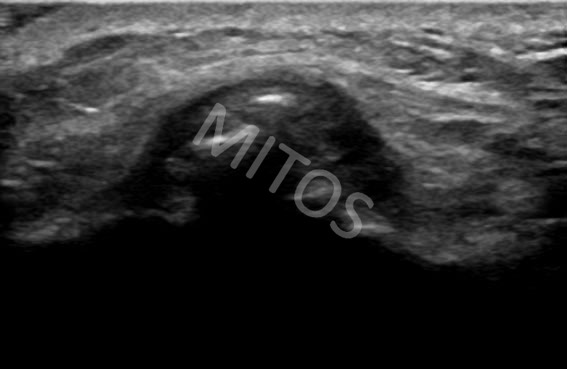
Along its course through the bicipital groove, the tendon of the LHB muscle is stabilized by various ligaments (the transverse humeral ligament, the coracobrachial ligament, the superior glenohumeral ligament) as well as by the Subscapularis tendon. Any pathology of the aforementioned anatomical structures leads to medial displacement of the LHB tendon (subluxation). It may be asymptomatic, (figure 2). Sonographically, in this case the normal LHB tendon is depicted laying over the Subscapularis muscle. The subluxation however, may accompany and complicate other pathological conditions in the shoulder area, mainly the partial or total rupture of the Subscapular tendon, (figure 3).
{kind=link}
{kind=link}
The bicipital groove is visualized “empty”.
Rupture (partial or total) of the LHB tendon
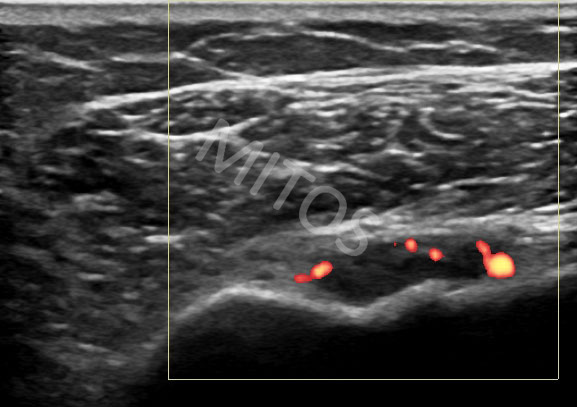
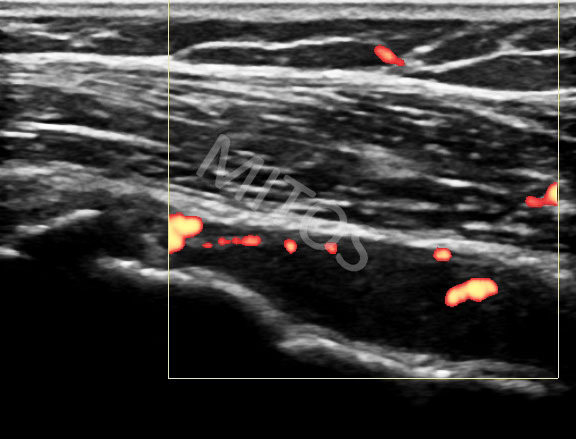
In the case of the LHB tendon recent rupture, the biceps groove is visualized with a content of mainly mixed echogenicity due to the presence of the empty inflamed tenontial sheath and the presence of debris within it, (figure 4a, figure 4b), with often positive Doppler signal (figure 5a, figure 5b), seen in two ultrasound planes.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
In oldstanding, established tears of the LHB tendon the bicipital groove appears “dry”, sometimes with presence of erosions at the bottom and pathological triangular deformation. The tenontial sheath merges with the surrounding fat and is not distinguished as a separate anatomical structure (figure 5g). All pathological findings are checked on both scanning planes.
{kind=link}
Bifid LHB tendon
Bifid LHB tendon is checked in both scanning planes. In transverse scan, (figure 6), two hyperechoic, oval structures are depicted, while in long scan two hyperechic, fibrillar structures that correspond to the separate tendons are visualized, (figure 7).
{kind=link}
{kind=link}
Rotator cuff pathology
Subacromial-subdeltoid bursa (SSDB)
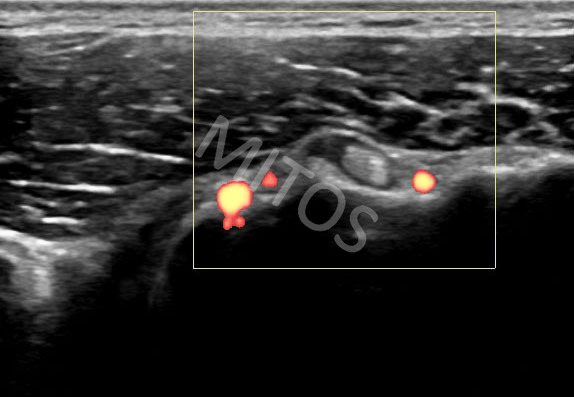
One of the most frequent pathological findings in the shoulder area is undoubtedly bursitis of the SSDB. Regardless of its causes, the affected bursa is visualized as an anechoic area of variable size and shape. Its pathology is often accompanied by tenosynovitis of the LHB, with a frequently positive Doppler signal, (figure 8).
{kind=link}
Calcific tendinitis
Almost all rotator cuff tendons present calcific tendinitis of varying degrees. On US, involved tendons are visualized as structures of an increased thickness and deranged echotexture.
The Supraspinatus tendon is most frequently affected. The appearance of present calcifications varies – from tiny, hyperechoic, needle-shape appearance without acoustic shadow, (figure 9), to a large, hyperechoic oval lesion in the middle of the tendon with an accompanying acoustic shadow, (figure 10).
{kind=link}
{kind=link}
Intratenontial calcifications are also frequently present in the tendon of the Subscapularis muscle, (figure 11).
{kind=link}
Tears
Tenontial tears are depicted in a view of anechioc lesions of various size, shape and location within the hyperechoic tenontial tissue. They may inflict more then one tendon in this region.
Tears should be evaluated in both sonographic planes (long and short).
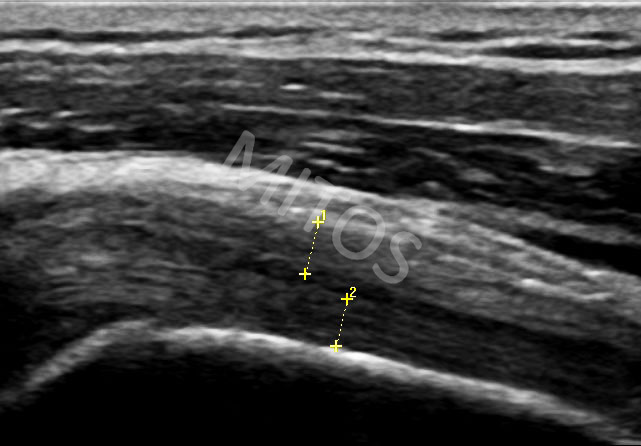
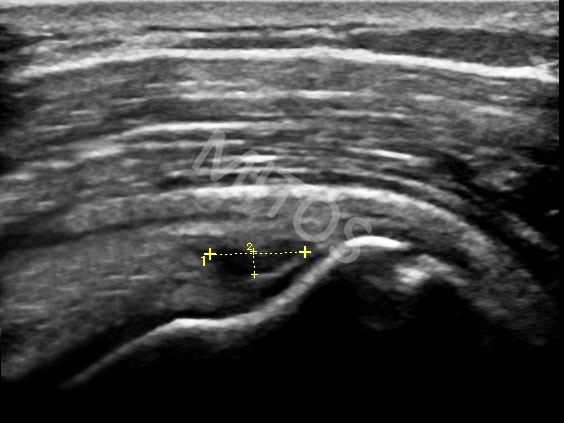
Τhe Supraspinatus tendon τears are most frequently seen in this region. They may be either a small, partial-thickness, (figure 12), or a large, full-thickness tear with tendon detachment and traction of the stump(s), (figure 13).
{kind=link}
{kind=link}
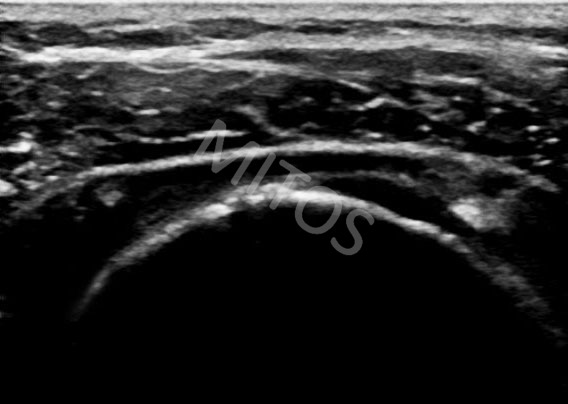
Sometimes, using the transverse US scan, a large intraparenchymal full-thickness tear with its communication with the SSDB and the cavity of the glenohumeral joint can be visualized, (figure 14).
{kind=link}
Erosions of the humeral head
Erosions of the humeral head are extremely common (even in asymptomatic individuals), underlying almost all tendons. When they are small, even multiple, they are considered of minimal importance, (figure 15a).
{kind=link}
From the other side, significant erosions are considered those that present a Doppler signal as an indication of activity. A typical case is a patient with Psoriatic arthritis and active, painful erosions present over the lesser humeral tubercle, (figure 15b, figure 15c).
{kind=link}
{kind=link}
Laterally to the LHB, especially in young individuals, the ascending branch of the anterior circumflex humeral artery is detected as a normal finding and should not be misinterpreted as a pathology of the region, (figure 15c ).
Pathology of the acromioclavicular joint (AC)
The AC joint frequently presents an image of osteoarthritis, (figure 16). It usually accompanies pathology of the glenohumeral joint and pathology of the rotator cuff tendons. Occasionally, calcium pyrophosphate depositions may be found within the fibrous AC discus, (figure 17).
{kind=link}
{kind=link}
Bibliography:
- Backhaus M, Burmester GR, Gerber T, Grassi W, Machoid KP, Swen WA, Wakefield RJ and Manger B. Guidelines for musculoskeletal ultrasound in rheumatology. Ann Rheum Dis 2001;60:641-49.
- Schmidt WA, Schmidt H, Schicke B, Gromnica-Ihle E. Standard reference values for musculoskeletal ultrasonography. Ann Rheum Dis 2004;63:988-94.
- Liu SH, Henry MH, Nuccion SL. A prospective evaluation of a new physical examination in predicting glenoid labral tears. Am J Sports Med 1996;24(6):721-5.
- Angelo R, Esch J, Ryu R. The shoulder: expert consult. Saunders Elsevier 2010.
- Crass JR, Craig EV, Feinberg SB. Ultrasonography of rotator cuff tears: a review of 500 diagnostic studies. J Clin Ultrasound 1998b;16:313-27.
- Middleton WD. Ultrasonography of the shoulder. Radiol Clin North Am 1992;30:927-40.
- Crass JR, Craig EV, Feinberg SB. The hyperextended internal rotation view in rotator cuff ultrasonography. J Clin Ultrasound 1987;15:416-20.
- Van Holsbeeck MT, Strouse PJ. Sonography of the shoulder: evaluation of the subacromial-subdeltoid bursa. AJR Am J Roentgenol 1993;160:561-4