


Ultrasound guided elbow injections
Ioannis Raftakis
One of the advantages of ultrasound is the possibility of performing guided injections either for diagnostic or therapeutic reasons. Elbow can be affected in inflammatory (rheumatoid, psoriatic arthritis, septic arthritis, gout) or mechanical conditions (tendinitis, rarely osteoarthritis).
With ultrasound accuracy, needle positioning is provided in order to aspirate or to inject a local treatment.1
Elbow joint injections
Elbow joint can be assessed either from the anterior or the posterior surface. A high frequency transducer (10-15MHz) is mandatory.
Material: A needle 23 or 25 G is adequate for aspiration. For therapeutic reasons 1 ml of lidocaine and 1 ml of beta-methasone, methylprednisolone or triamcinolone is needed.
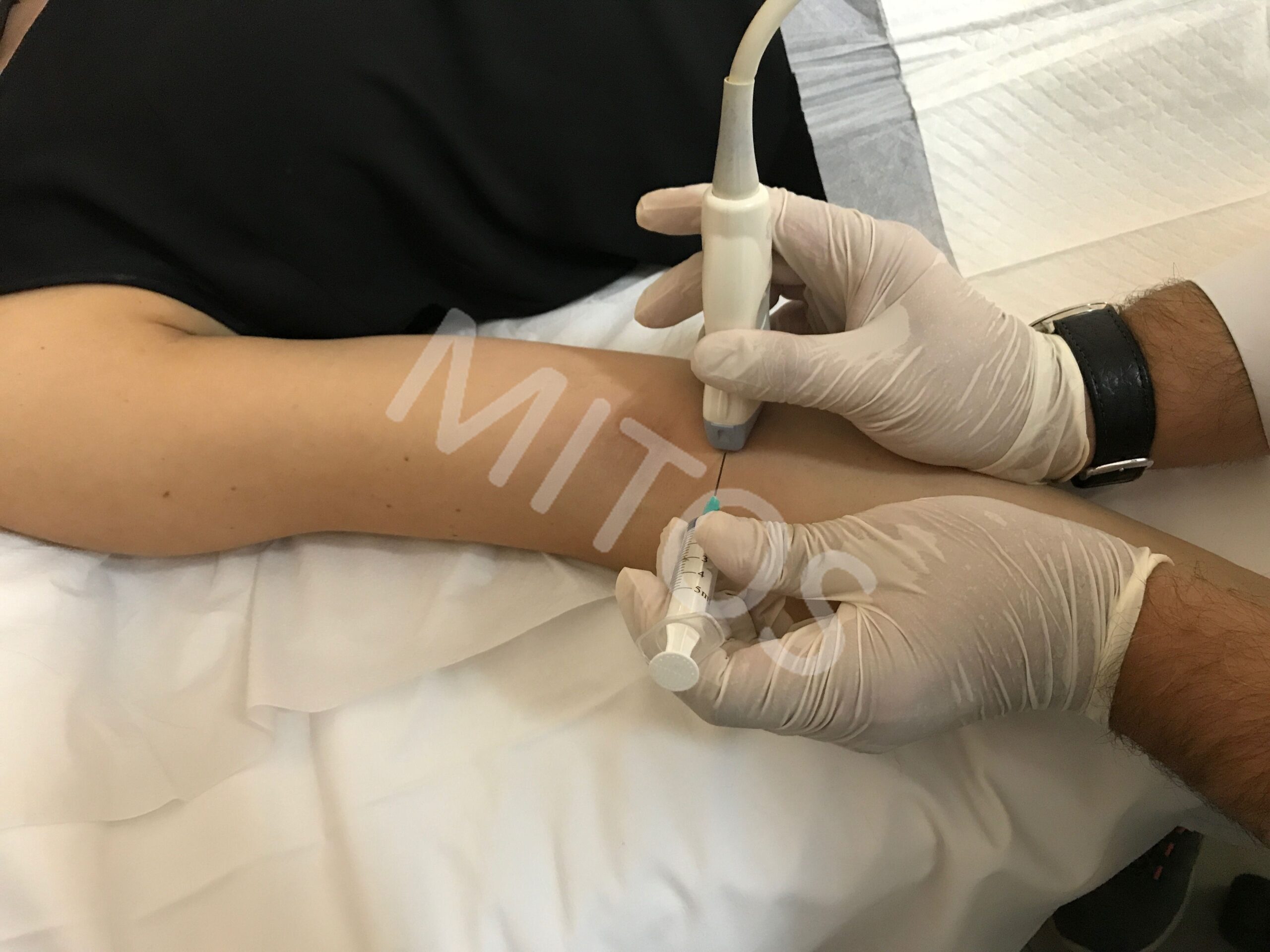
Patient positioning: For anterior injections the patient can be placed in prone position, with the elbow flexed 45-90° and placed overhead, forearm in pronation with palms facing down (figure 1).
{kind=link}
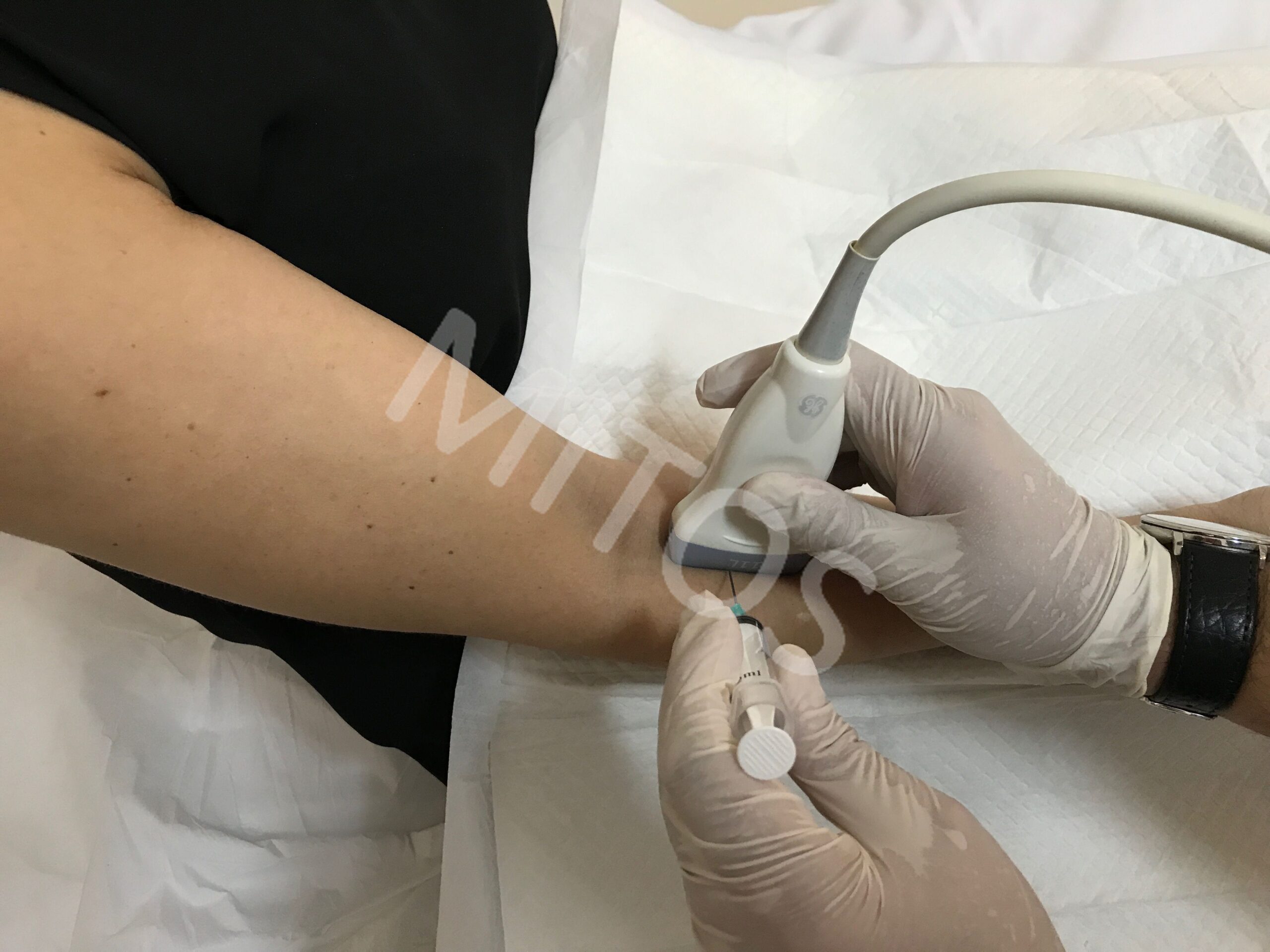
Procedure: The probe is placed parallel to the brachioradial joint, in line with radial bone. Needle is placed parallel to the probe aiming the intra-articular space. Alternatively, the probe is kept in the same position, but the needle is oriented perpendicular to it. In this case we can see only the tip of the needle (figure 2).
Patient positioning for posterior approach: This is performed in cases of fluid collection in the olecranon recess. The patient is in prone position, elbow flexed in 90° and the forearm hanging from the examination bed (figure 3).
{kind=link}
Procedure: The probe is placed perpendicular to the triceps tendon and the needle is also placed parallel to the probe. The orientation is from the lateral to the medial aspect, in order to avoid the ulnar nerve. An alternative could be by placing the needle parallel to the probe, by assuming a more lateral positioning, as to not harm the triceps tendon.
Lateral epicondyle injections
This is the origin of the common extensor tendon, which is formed by the extensor carpi radials, extensor carpi ulnaris, common extension digitorum and the extensor digiti minimi.
Indications: Tendinitis of the common extension tendon, known as lateral epicondylitis, can be due to repeated micro trauma. Enthesitis is also common in seronegative Spondylarthritis.
Material: 1ml of lidocaine and 1 ml of steroids is adequate in cases whether all other treatments have failed.
Patient positioning: The patient is in supine or rarely in seated position withe the arm and the wrist in pronation (figure 4).
Procedure: The probe is placed parallel to the common extensor tendon and the needle parallel to the probe. The orientation of the needle is from the distal to the proximal part. Alternatively, the patient is in the same position, but the probe is placed perpendicular to the tendon origin. The needle is also placed parallel to the probe directed from the posterior to the anterior aspect (figure 5).
Pearl: The injection must be performed to the peritendinous area and not directly to the tendon.
Medial epicondylitis injection
This is the origin of the flexor common tendon formed by the pronator teres, flexor carpi ulnaris, flexor carpi radials, palmaris longus, and flexor digitorum superficialis.
Indications: Tendinitis of the common flexor tendon, known as golfers elbow, although less common than the lateral one, can also be due to repetitive micro trauma. Enthesitis can also occur. Medication is the same as for lateral epicondylitis.
Patient positioning: The patient is placed in supine position elbow flexed 90° and the wrist in supination (figure 6).
Procedure: The probe is placed parallel to the tendon and the needle parallel to the probe, aiming from the distal to the proximal part. Alternatively the probe is placed perpendicular to the tendon and the needle parallel to to the robe. The orientation of the needle is from the anterior to the posterior surface (figure 7).
Pearl: Again caution should be taken to inject the peritendinous area and try to avoid the ulnar nerve.
Injection of the olecranon bursa
The olecranon bursa lies superficially between skin and the olecranon and does not communicate with the joint.
Indications: Olecranon bursitis can be due to either trauma, infection, or as an additional sign of a systemic rheumatic disease.
Material: For aspiration a 18G needle is adequate. For injections, 0.5 ml de lidocaine and 0.5-1 ml of steroids are also adequate.
Patient positioning: The patient is either in supine position with the shoulder in internal rotation and 30° of flexion, or in prone position with shoulder in abduction and elbow in flexion, as forearm hanging from the examination table (figure 8).
Procedure: The probe can be placed parallel or perpendicular to the bursa and the needle parallel to the probe.
Injections of the distal biceps tendon and bicipitoradial bursa
Although rare, distal biceps tendon can be affected due to repetitive trauma and it is common in weight lifters. Even rarer is the presence of bicipitoradial bursitis in patients with a systemic rheumatic disease.
Indications: Persistent pain, not responding to other treatment.
Material: A 25G needle will be needed as well as 2 ml of lidocaine and 0.5-1 ml of steroids.
Patient positioning: The best position is with the patient supine, elbow flexed and hyper pronation of the forearm (figure 9).
Procedure: The probe is placed perpendicular to the posterior aspect of the forearm, 3-4 cm distal to the olecranon. The needle is parallel to the probe from the radial to the ulnar side.
Pearl: Once more caution should be taken to avoid directly injecting the tendon.
Ulnar nerve injections
Ulnar nerve can be affected in his groove due to increased pressure from repetitive micro trauma, fractures which give a thickened appearance in ultrasound.
Indications: Pain at the ulnar groove and numbness of the half 4 and 5th finger.
Material: A 25 G needle, 2 ml of lidocaine and 0.5-1 ml of steroids are adequate.
Patient positioning: The patient is in supine position with slight abduction and supination of the forearm (figure 10).
Procedure: The probe is placed perpendicular to the nerve. The needle is parallel to the probe and the orientation can be either from the lateral or from the medial surface.
If the nerve is compressed more centrally the arm is in 90° of abduction and forearm in pronation. The technique remains the same (figure 11).
Pearl: Extreme caution is needed in order not to touch the nerve it self.
Median nerve injections
Although less common than carpal tunnel syndrome, the median nerve can be compressed also at the elbow at the level of pronator teres muscle.
Indication: Pain and numbness originating from this area.
Material: A 25G needle, 2ml of lidocaine and 0-5-1 ml of steroids may be used.
Patient positioning: The patient is in supine position with the forearm in extension and supination (figure 12).
Procedure: The probe is placed parallel to the nerve and the needle parallel to the probe. The orientation is from the distal to the proximal part. Alternatively the probe is perpendicular to the nerve and the needle parallel to the probe, aiming the nerve from the lateral to the medial surface, between the two heads of pronator teres muscle (figure 13).
{kind=link}
Pearl: Using Power or Color Doppler can help avoiding injecting a vessel. Again caution no to touch the neve itself.
Posterior interosseous nerve injections
The deep branch of the radial nerve can be compressed at the level of the supinator muscle, in the arcade of Frohse. Clinical manifestations may resemble those from lateral epicondylitis.
Indications: Persistent pain originating from this area, confirmation by ultrasound of the pathology and if there is failure of symptomatic treatment.
Material: A needle 23-25 G, 2 ml of lidocaine and 0.5-1 ml of steroids are needed.
Patent positioning: The patient is in supine position, or seated with the forearm resting on the examination tube and the thumb pointing upwards (figure 14).
{kind=link}
Procedure: The probe is placed perpendicular to the nerve and the needle parallel to the robe. The orientation is from the lateral to the medial aspect.
Pearl: Once more caution should be taken to avoid the nerve itself.
Bibliography:
- Cardone DA, Tallia AF. Diagnostic and therapeutic injection of the elbow region Am Fam Physician 2002; 66( 11) : 2097-2100
- US-guided injection of the upper and lower extremity joints. Collins JM, Smithuis R, Rutten MJ. Eur J 2012 Oct;81(10):2759-70
- Micheo WF Rodriquez RA, Amy E. Joint and soft tissue injections of the upper extremity. Physical Medicine and rehabilitation Clinics of North America Philadelphia PA Saunders 1995: 830-832
- Regan WD, et al: Tendinopathies around the elbowIn. Delee JC et al. Delee and Dreze’ sOrthopaedic Sports Medicine 3 rd edition Philadelphia PA: Saunders 2009
- Kalume Brigito M et al: Improved visualisation of the radial insertion of the biceps tendon at ultrasound with a lateral approach Our Radiol 2009; 19(8): 1817-1821
- Okamoto M, Abe M, Shirai H et al: Morphology and dynamics of the ulnar nerve in the cubital tunnel: observation by ultrasonography. Hand Sure Br 2000; 25( 1) 85-89
- Grutter P et al: The accuracy of distal posterior interosseous and anterior interosseous nerve injection. J Hand Surg Am 2004;29(5):865-870
Ultrasound guided shoulder injections
Ioannis Raftakis
Shoulder can be affected either due to an inflammatory process (rheumatoid arthritis, septic arthritis), or due to degenerative couses. Pathology may be localized at the tendons or the bursae as well. Ultrasound can accurately define the pathology and guide aspiration or injection of steroids.
Injections of the glenohumeral joint
This procedure may be used either to aspirate synovial fluid in order to rule out an infectious process, or guide intraarticular treatment.
Material: A medium frequency transducer, a long needle 21-23 G (as a lumbar spine needle), 5-10ml of local anaesthetic and 1 ml of steroids (triamcinolone, beta-methadone or methylprednisolone) are needed.
Patient positioning: The patient is in supine lateral position on the contralateral side, (figure 1).1
{kind=link}
Procedure: The probe is placed parallel to the infraspinatus tendon and the needle is also parallel to the probe, aiming the joint line.
Pearl: Caution should be taken in order to avoid the articular cartilage. A small amount of fluid may be introduced to verify the exact positioning of the needle, as to reorientate it if necessary.
Alternatively the patient may be in supine position with the arm is slight external rotation aiming the anterior part of the joint from the external to the internal aspect (figure 2).
{kind=link}
Procedure: The probe gets parallel to the anterior aspect of the joint and the needle parallel to the probe from the external to the internal part. Arm positioning in external rotation helps to better visualise the needle.2
Injection of the subacromial-subdeltoid bursa
Subacromial bursitis is a common cause of shoulder pain. Usually it is the result of shoulder impingement, but sometimes it can be inflamed in the course of a systemic inflammatory disease.
Indications: Persistent pain, not responding to other treatment, or for diagnostic purposes
Material: A 25 G needle is adequate. For injection 1 ml of local anaesthetic and 1ml of steroids will be needed.
Patient positioning: The patient can be in supine position or lying on the controlateral side, (figure 3).
Procedure: The probe is placed parallel or transversely to the bursa depending on the best visualisation. The needle it self is also placed parallel to the probe oriented from the external to the internal aspect.3
Injections of the subcoracoid bursa
The bursa overlies the subscapularis tendon. It can rarely be affected in cases of impingement syndrome, or accompany tears of the rotator cuff.
Indications: Persistent pain not responding to other treatment
Material: Similar to those used for the subacromial bursa.
Patient positioning: The patient lies in supine position with the shoulder in external rotation, (figure 4).
Procedure: The probe is set parallel to the subscapularis tendon and the needle parallel to the probe. The orientation is from the external to the internal aspect.
Doppler modality may be used to avoid vascular structures.4
Injections of the long biceps tendon
Tenosynovitis of the biceps tendon is mainly a sign of glenohumeral synovitis of any aetiology. Ultrasound injections provide much accuracy in contrast with the blind ones.
Indications: Persisting inflammation not responding to other treatment.
Material: A23-25G needle, 0.5 ml of anaesthetic and 1 ml of steroids are adequate.
Patient positioning: The patient lies in supine position, (figure 5).
Procedure: The needle is placed transversely to the tendon and the needle parallel to the probe oriented from externally to internally.
Pearl: Caution in needed to avoid injecting the tendon itself. Doppler can be used to avoid also vascular structures.
Alternatively with the patient in the same position, the probe can be placed parallel to the tendon, the needle parallel to the probe. The orientation is from cranial to the distal part of the tendon, (figure 6).5
Injections for calcific tendinitis
Rotator cuff tendons and especially the supraspinatus tendon, may be affected by calcific tendinitis, either to repeated micro trauma or either due to diabetes, thyroid disease or ageing.
Indications: Persistent pain not responding to conservative treatment or contra-indication to NSAIDS.
Material: A23-25G needle, 0.5 ml of anaesthetic and 1 ml of steroids are adequate.
Patient positioning: The patient is in supine position or lying to the contralateral side (figure 7).
Procedure: The probe is placed parallel to the affected tendon and the needle is also parallel to the probe aiming from the external to the internal aspect.
Barbotage is a technique applied under local anaesthesia, aiming at breaking down the calcific deposits, local lavage and aspiration of calcific fragments.6
Injections of the supra scapular nerve
The nerve originates from the A5-6 roots and rarely in case of impingement (ganglion cyst) it might cause pain and loss of muscular strength and atrophy of supraspinatus and infraspinatus muscles.
Indications: Pain originating from the nerve, presence of a ganglion cyst or atrophy of the affected muscles.
Material: A lumbar spine needle will be needed with 4-5 ml of anaesthetic and 1 ml of steroids.
Patient positioning: The patient is seated, with the palm on the contralateral shoulder (figure 8).
Procedure: The probe is placed transversely, obliquely, parallel to the spine of the scapula. The needle is also parallel to the probe with orientation either from the lateral or the medial side.
Pearl: Caution is needed to avoid harming the nerve.7
Injections of acromiovlavicular joint
The joint may be affected due to osteoarthrits, rheumatoid arthritis or trauma. Although there might be no difference in relieving pain comparing guided or blind injections, in case of advanced osteoarthritis, ultrasound is helpful to accurately place the needle.8
Indications: Persistent inflammation, not responding to other treatments.
Material: A 25 Needle with 0.5-1ml of anaesthetic and 0.5-1 ml of steroids will be needed.
Patient positioning: The patient can be sited or lying in supine position (figure 9).
Procedure: The probe is placed transversely and obliquely to the joint and the needle transversely to the probe.9
Alternatively the probe is transversely to the anterior aspect of the joint and the needle parallel to the probe, from the anterior to the posterior aspect, (figure 10).
Injections of the sternoclavicular joint
The joint may be affected due to trauma, in case of inflammatory conditions (SAPHO syndrome) and rarely to infectious agents especially in toxic drug addicts.
Indications: Alleviating pain or for diagnostic purposes.
Material: A 23-25G needle, 0.5 ml of anaesthetic and 1 ml of steroids are adequate.
Patient positioning: The probe is placed parallel and obliquely to the joint and the needle parallel to the probe from internally to externally, (figure 11).
Alternatively the probe can be placed transversely and obliquely to the joint and the needle aiming cranial, (figure 12).
Pearl: Caution is needed no to exceed the joint margins.10
Bibliografy:
- Carl P.C.Chen et al: Ultrasound guided Glenohumeral Joint Injection using the posterior approach. Am J Phys Med Rehabil 2015Dec; 94(12): e117–e118.
- Zwar R et al: Sonographically guided glenohumeral joint injection. AJR Am J Roentgenol.2004:48-50
- Ultrasound-guided shoulder injections in the treatment of subscromial bursitis. Am J Phys Med Rehabil. 2006;85(1) 31-35
- Mens J et al: Calcifying subcoracoid bursitis as a cause of chronic shoulder pain. Ann Rheum Dis 1984;43:758-759
- Zhang J et al: Ultrasound-guided injection for the biceps brachii tendinitis: results and experience. Ultrasound Med Biom; 2011(5):729-733
- Niazi G et al:The role of ultrasound guided percutaneous needle aspiration and lavage (barbotage) in the treatment of calcific tendinitis. The Egyptian Journal of Radiology and Nuclear Medicine 2015 46(1):63-70
- Harmon D et al: Ultrasound-guided supra scapular nerve block technique. Pain Physician. 2007Nov;10(6):743-746
- Sabeti-Aschraf M et al: The infiltration of the AC joint performed by one specialist: ultrasound versus palpation a prospective randomised pilot study. Our JRadiol.2010;75(1)e37-e40
- Sabeti-Aschraf M et al: Ultrasound guidance improves the accuracy of the AC joint infiltration: a prospective randomised study. Knee Sure Sports Traumatol Arrthrosc. 2011Feb;19(2):292-295
- Weinberg AM et al: Frequency of successful intra-articular puncture of the sternoclavicular joint. A cadaver study Scand J Rheumatol 2009;38(5):396-398