


HIP
Giasna Giokits (Jasna Jokic)
The hip joint is frequently affected by inflammatory arthritis, degenerative diseases or injuries. Additionally to the careful clinical examination, the detailed personal and family history as well as the appropriate blood tests application of imaging methods is absolutely necessary.
Undoubtedly, the most important indication of the hip joint evaluation with ultrasound (US) is finding of the fluid collection in the joint synovial cavity itself or within the tenondial and ligamentous structures in inflammatory, degenerative, infectious or traumatic processes.
The pathologies that can be detected by US are:
- Presence of fluid within the synovial cavities of the hip joint with the possibility of finding even minimal amounts of fluid. Various cystic lesions can be found as well. In addition, use of US allows easy and efficient application of therapeutic injections.
- Evaluation of the synovial thickening.
- Detection of partial or total rupture of ligaments and tendons.
- Imaging of bone contour changes (osteophytes, erosions).
- Detection of the articular cartilage pathology (e.g. crystal depositions, changing of the cartilage thickness or echogenicity). Pathology of the fibrous labrum can be detected as well.
For optimal imaging of the hip joint, due to its deep location, a 3.5-5 MHz convex transducer is used, especially in obese patients. Alternatively, in slim patients, a low-frequency (≤7 MHz) linear transducer can be used.
In general, pathology of the hip area may be found in the joint itself, within the surrounding soft tissues, as well as in the soft tissues (tendons and bursae) that surround the great trochanteric area.
According to the EULAR guidelines there are four standard scans that allow full evaluation of the hip joint.
Synovitis of the hip joint
The collection of fluid within the synovial joint cavity of the hip joint is the most common finding seen by US. The hip synovitis may be presented due to almost all possible pathological conditions that can affect the hip area such as degenerative, inflammatory and post-traumatic arthritides.
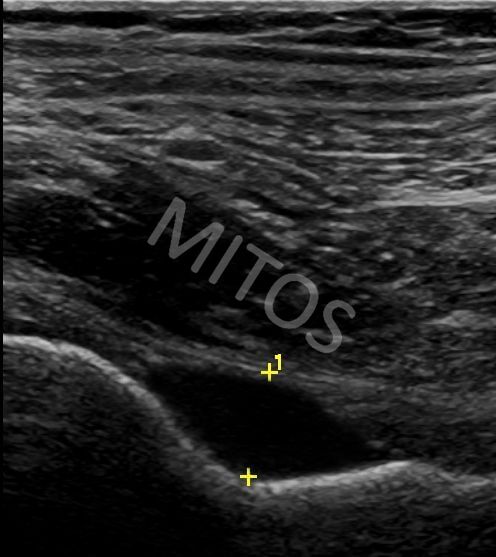
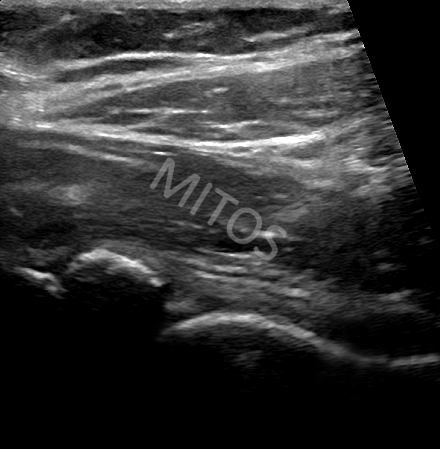
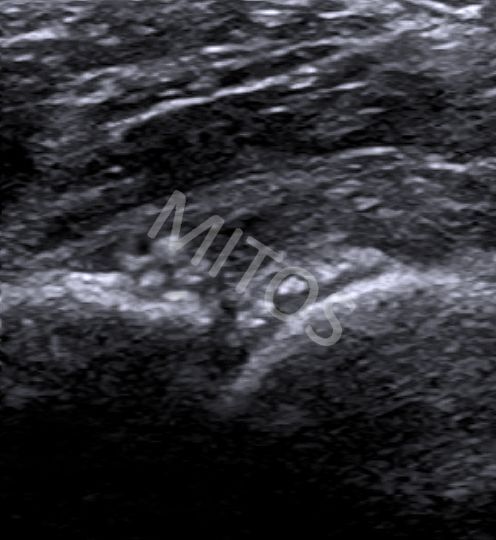
In the case of patient with rheumatoid arthritis (RA), during the ultrasound imaging of the hips, an amount of fluid inside the joint cavity can be found in a view of anechoic area in close proximity to the femoral neck, (figure 1a), compared to the normal ultrasound image, (figure 1b). In case of late RA, erosions of articular cartilage can also be found, (figure 1c).
{kind=link}
{kind=link}
{kind=link}
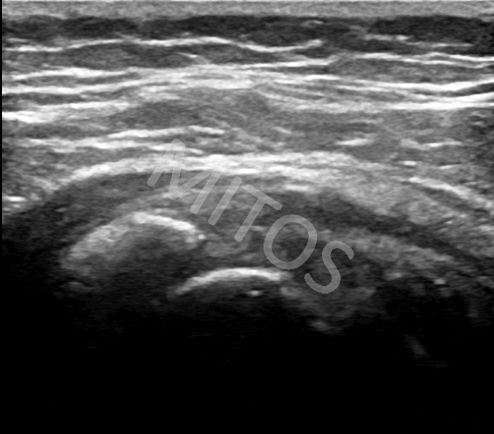
US image of post-traumatic hip osteoarthritis, usually differs from the image found in patients with inflammatory diseases. Fluid collection within the joint cavity is typically of mixed echogenicity (mainly hypo/anechoic) due to the presence of debris, (figure 1d). The synovial layer is frequently hypertrophied. The bony contour of the femoral head is presented with an abnormal “step-up” bony prominence due to the presence of osteophytes.
{kind=link}
MRI is undoubtedly the method of choice for detecting of osteonecrosis. However, during the US evaluation of hip osteonecrosis, in addition to the presence of effusion (usually of mixed echogenicity due to the presence of debris) within the joint cavity, US can highlight the femoral head bony contour breakdown, (figure 1e). This might be supportive to diagnosis.
{kind=link}
The use of US as a diagnostic method is gaining more and more space in pediatric Rheumatology. In the case of a four-year-old child with persistent hip lameness, an amount of fluid within the slightly hypertrophic synovial membrane is found during the US examination, (figure 1f).
{kind=link}
Crystal induced arthropathy
The area of the hip joint is easily evaluated for the possible presence of crystal deposits. During the US examination of a painful hip in a patient with chronic CPPD arthropathy, a large CPP deposits is found in the area of the fibrous labrum, (figure 2a).
{kind=link}
In a patient with long-standing CPPD arthropathy, typical deposits of CPP crystals within the femoral head hyaline cartilage (chondrocalcinosis) are depicted. Additionally, punctuate scattered deposits within the fibrous labrum are seen, (figure 2b).
{kind=link}
US examination of a patient with chronic gout and frequent flares, despite systemic therapy, reveals typical monosodium urate crystal deposits over the femoral head hyaline cartilage surface, creating a “double contour sign” image. Scattered, punctate monosodium urate crystal deposits within the fibrous labrum are visualized as well, (figure 2c).
{kind=link}
Pathology of the iliopsoas bursa
Under normal conditions, the iliopsoas bursa is not visualized by US, due to the minimal or no amount of fluid within its cavity. In case of the hip synovitis, if the iliopsoas bursa communicates with the joint cavity, synovial fluid enters into the bursa creating typical US image of bursitis. Bursitis of the iliopsoas bursa can be also found as a separate pathology of the area in degenerative and post-traumatic cases.
In case of hip osteoarthritis, a hypoechoic structure, which communicates with the joint cavity, is visualized. This lesion extends between the neurovascular bundle (medially) and the iliopsoas muscle (laterally). The inflamed iliopsoas bursa should be checked in two perpendicular planes (transverse and longitudinal), (figure 3a, figure 3b).
{kind=link}
{kind=link}
Pathology of the greater trochanteric area
US very often shows pathological findings of the gluteus medius tendon (of the superficial part, attached over the broad outer surface of the greater trochanter and its deep part inserted on the postero-superior surface of the greater trochanter upper pole).
An enlarged and hypoechoic tendon of the gluteus medius muscle is typically seen in the region near its epiphysis, (figure 4).
{kind=link}
In the case of severe pain over the area of the greater trochanter, with aggravation during the night and lying down, US sometimes shows scattered calcifications of varying sizes within the tendon of the gluteus medius muscle near the insertion to the greater trochanter, (figure 5a, Figure 5b).
{kind=link}
{kind=link}
Bibliography:
- Bruyn GA, Schmidt WA. Introductory Guide to Musculoskeletal Ultrasound for the Rheumatologist 45-56 p.
- Bianchi S, Martnoli C. Ultrasound of the Muskuloskeletal System 2007. 551-611 p.
- Backhaus M. Ultrasound and structural changes in inflammatory arthritis: synovitis and tenosynovitis. Ann N Y Acad Sci 2009;1154:139-51.
- Pauroso S, Di Martino A, Tarantino CC, Capone F. Transient synovitis of the hip: Ultrasound appearance. Mini-pictorial essay. Journal of Ultrasound 2011;14(2):92-4.
- Kang YR, Koo J. Ultrasonography of the pediatric hip and spine. Ultrasonography 2017;36(3):239-51.
- Nestorova R, Vlad V, Petranova T, Porta F, Radunovic G, Micu MC, et al. Ultrasonography of the hip. Med Ultrason 2012;14(3):217-24.
- Park KD, Lee WY, Lee J, Park MH, Ahn JK, Park Y. Factors Associated with the Outcome of Ultrasound-Guided Trochanteric Bursa Injection in Greater Trochanteric Pain Syndrome: A Retrospective Cohort Study. Pain Physician 2016;19(4):E547-57.
- Molini L, Precerutti M, Gervasio A, Draghi F, Bianchi S. Hip: Anatomy and US technique. Journal of Ultrasound 2011;14(2):99-108.
- Wunderbaldinger P, Bremer C, Schellenberger E, Cejna M, Turetschek K, Kainberger F. Imaging features of iliopsoas bursitis. Eur Radiol 2002;12(2):409-15.
- Johnston CA, Wiley JP, Lindsay DM, Wiseman DA. Iliopsoas bursitis and tendinitis. A review. Sports Med 1998;25(4):271-83.
- Long SS, Surrey DE, Nazarian LN. Sonography of greater trochanteric pain syndrome and the rarity of primary bursitis. AJR Am J Roentgenol 2013;201(5):1083-6.
- McEvoy JR, Lee KS, Blankenbaker DG, del Rio AM, Keene JS. Ultrasound-guided corticosteroid injections for treatment of greater trochanteric pain syndrome: greater trochanter bursa versus subgluteus medius bursa. AJR Am J Roentgenol 2013;201(2):W313-7.
- Bierma-Zeinstra SMA, Bohnen AM, Verhaar JAN, Prins A, Ginai-Karamat AZ, Laméris JS. Sonography for hip joint effusion in adults with hip pain. Annals of the Rheumatic Diseases 2000;59(3):178-82.
- Stoica Z, Dumitrescu D, Popescu M, Gheonea I, Gabor M, Bogdan N. Imaging of Avascular Necrosis of Femoral Head: Familiar Methods and Newer Trends. Current Health Sciences Journal 2009;35(1):23-8.
- Miksanek J, Rosenthal AK. Imaging of Calcium Pyrophosphate Deposition Disease. Current rheumatology reports 2015;17(3):20-23.
- Frediani B, Filippou G, Falsetti P, Lorenzini S, Baldi F, Acciai C, et al. Diagnosis of calcium pyrophosphate dihydrate crystal deposition disease: ultrasonographic criteria proposed. Ann Rheum Dis 2005;64(4):638-40.
- Magarelli N, Amelia R, Melillo N, Nasuto M, Cantatore F, Guglielmi G. Imaging of chondrocalcinosis: calcium pyrophosphate dihydrate (CPPD) crystal deposition disease — imaging of common sites of involvement. Clin Exp Rheumatol 2012;30(1):118-25.
- Forien M, Combier A, Gardette A, Palazzo E, Dieude P, Ottaviani S. Comparison of ultrasonography and radiography of the wrist for diagnosis of calcium pyrophosphate deposition. Joint Bone Spine
- Huet T, Ottaviani S, Coustet B, Dieude P. Hip Gout Arthritis Revealed by Sonography. J Ultrasound Med 2016;35(8):1828-9.
- Rowbotham EL, Grainger AJ. Ultrasound-Guided Intervention Around the Hip Joint. American Journal of Roentgenology 2011;197(1):W122-W7.