


WRIST AND HAND
Dimitrios Karokis
Pathological findings of the wrist joint
Synovitis
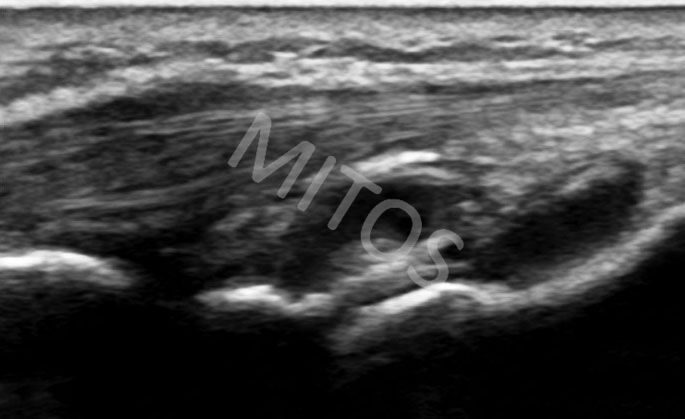
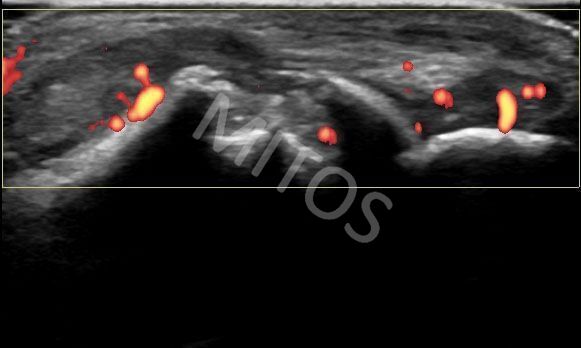
Synovitis is the most frequent finding in clinical practice, regardless of etiology. It is usually found in cases of inflammatory arthritis but also in other diseases such as systemic lupus erythematosus and Sjogren’s syndrome. An intra-articular fluid collection, (figure 1a), appears as an anechoic or hypoechoic area that may be compressed and displaced by transducer pressure. If the Power Doppler mode is applied, the Power Doppler signal will be restricted only to the synovial tissue, (figure 1b).
{kind=link}
{kind=link}
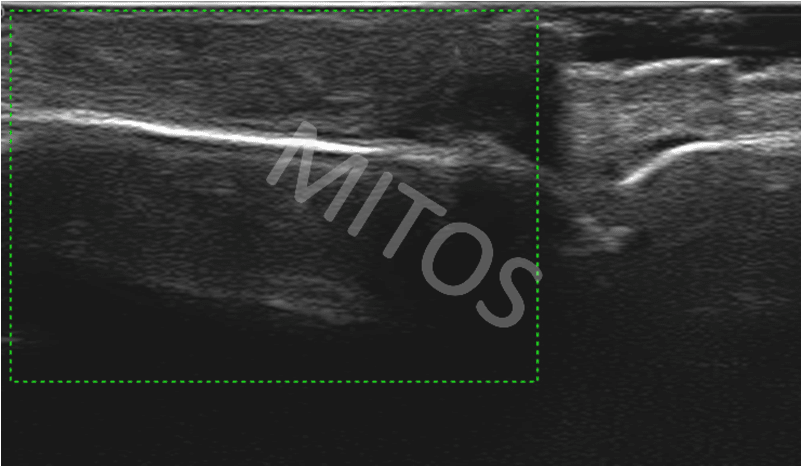
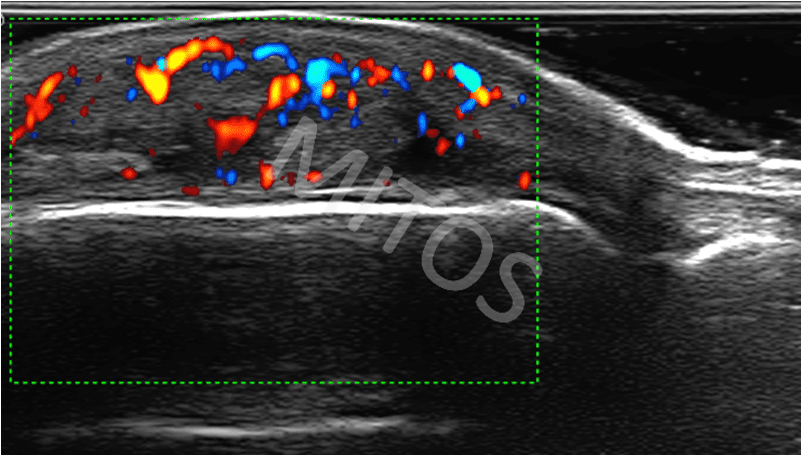
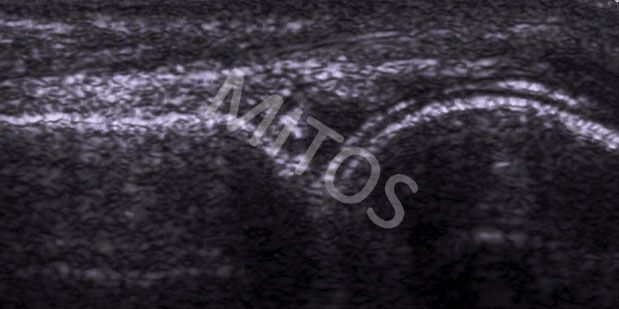
Synovial hypertrophy appears as a hypoechoic lesion that can’t be significantly displaced or compressed by transducer pressure, (figure 2a) and may show signal on Power or Color Doppler examination, (figure 2b).
{kind=link}
{kind=link}
In active synovitis, additionally to positive Power Doppler signal within the synovial wall, tenosynovitis of the extensor tendons may coexist. Extensor tendons may be surrounded by an anechoic hallo that corresponds to the presence of fluid or/and by hypoechoic swollen sheath that may express positive Power Doppler signal due to inflammation.
Ultrasound can be used for the quantitative and semi-quantitative scoring of inflammation.
There is considerable debate and arguing about the utility of US in detection of subclinical synovitis and whether it should determine the monitoring and treatment of these patients.
Erosions
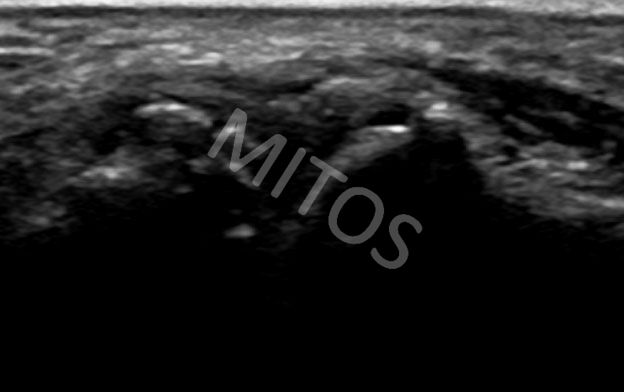
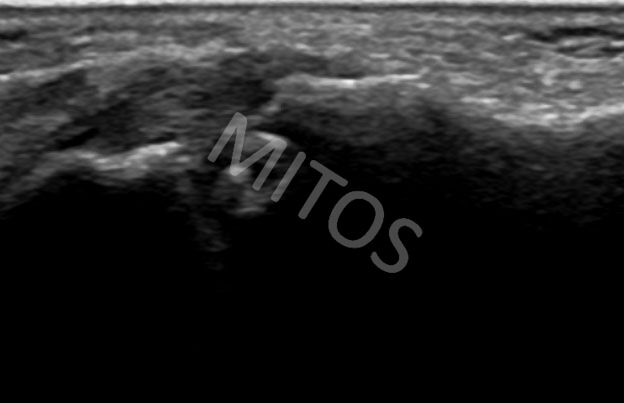
Erosion is bone pathology defined as a discontinuity of the bone cortical surface seen in two perpendicular planes. US has been proved as a more sensitive method than plain radiography in the early detection of erosions. Recent erosions appear with irregular borders and indistinct bottom, (figure 2c). In active RA synovitis, positive Power Doppler signal can be detected within the erosion area, (figure 2d).
{kind=link}
{kind=link}
Tenosynovitis
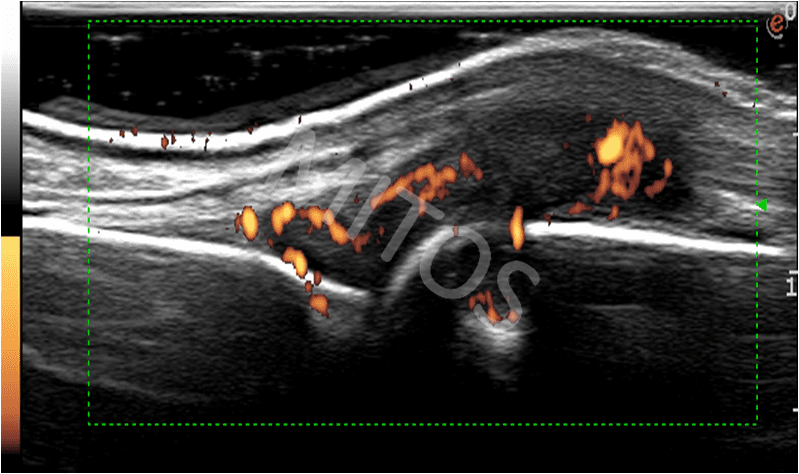
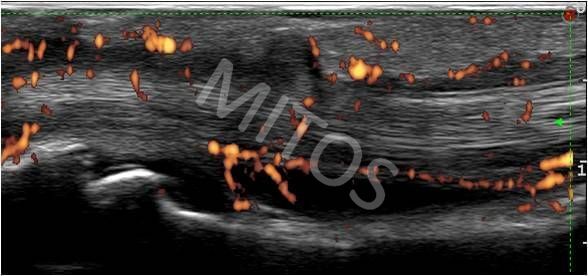
Flexor tendonitis / tenosynovitis is frequently found in patients with inflammatory arthritis such as RA (in 65-94% of patients), psoriatic arthritis and crystal induced arthritides, but also in bacterial infections, diabetes mellitus, amyloidosis and osteoarthritis, as well as in injuries and overuse syndromes. US tenosynovitis is defined as the presence of hypoechoic tissue that surrounds the hyperechoic tendon cross-section that might be accompanied with anechoic fluid collection in between two aforementioned structures. These findings may also show positive Power Doppler signal, (figure 3).
{kind=link}
In tendons that are not invested with synovial sheath, paratendinitis is defined as the presence of a hypoechoic hallo surrounding the tendon, possibly with positive Power Doppler signal.
At the level of the carpal tunnel, fluid collection can cause compression of the median nerve, causing symptoms and signs of secondary carpal tunnel syndrome, (figure 4). In patients with active inflammation, a positive Power Doppler signal may also be detected.
{kind=link}
De quervain tenosynovitis is inflammation of the tendons of the 1st extensor’s compartment (abductor pollicis longus and extensor pollicis brevis), seen along the lateral aspect of the radial bone. It causes pain over the styloid process area, typically aggravated by lifting heavy objects. Sonographically, the typical disruption of normal tendon morphology (swelling of the tendons and their focal or diffuse hypoechogenicity) is usually seen, (figure 5a). Positive Power Doppler signal may coexist, (figure 5b).
{kind=link}
{kind=link}
Carpal tunnel syndrome
Carpal tunnel syndrome (CTS) is the most common entrapment neuropathy. Typical symptoms in CTS is perception of numbness and burning of the lateral side of the hand and the first three fingers, mainly at night. During the day a patient may experience the same symptoms when holds objects for a long time keeping the hands at the same position. CTS is invoked by compression of the median nerve (MN) at the level of the carpal tunnel and can be either primary (most commonly due to overuse) or secondary, due to acute inflammatory arthritides or other causes, such as flexor tendonitis, uric acid deposition, amyloid or ganglion.
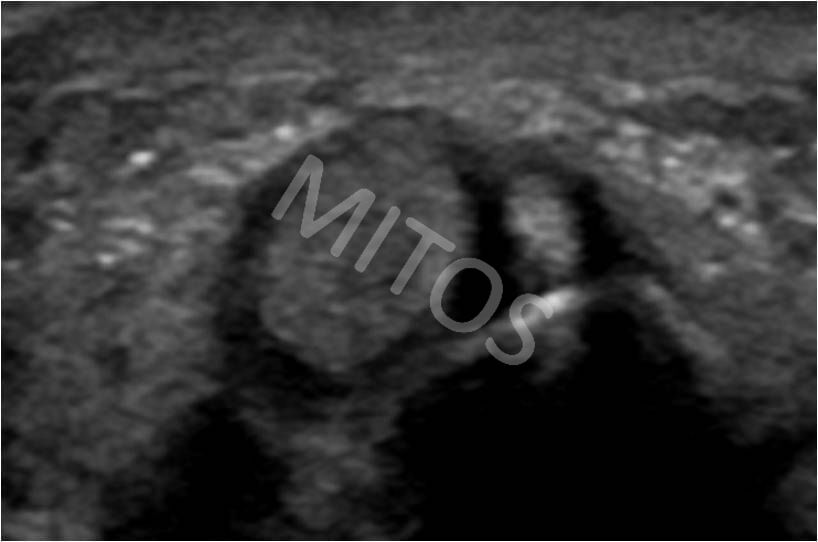
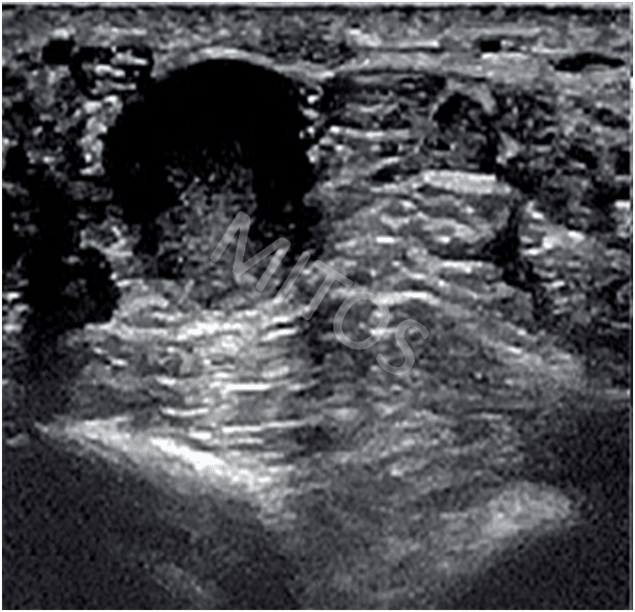
Different kind of tumors (e.g. Schwanoma) may also invoke CTS. Schwanoma is characteristically visualized in longitudinal, (figure 6a) and transverse plane, (figure 6b).
{kind=link}
{kind=link}
The MN in CTS, examined by US at the level of the distal pole of the ulna or at the entrance of the carpal tunnel, is typically swollen and the transverse carpal ligament becomes more convex due to the pressure of the CT content. The affected MN may express positive Doppler signal. In the CTS, the cross-section of the MN is hypoechoic and enlarged (area >10 mm2 and up to 30 mm2 is considered as patognomonic for the CTS), (figure 6c).
{kind=link}
Ganglia
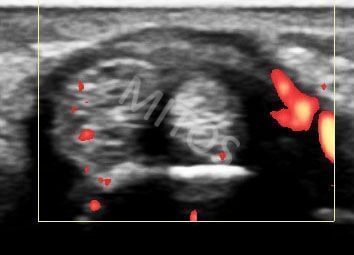
Ganglia are the most common cystic lesions in the wrist and hand area. They contain viscous sticky liquid encased within a fibrous capsule. Most ganglia (60-70%) are located on the dorsal surface of the wrist. They also may be located on the carpal side of the wrist, (figure 7), at the base of the fingers, near the flexor carpi radialis tendon and within the CT.
{kind=link}
Simple ganglion cysts appear as well-circumscribed, lobulated, hypo or anechoic lesions, possibly presenting thin septa in their cavity. Long-standing ganglion cysts may show increased echogenicity, thick internal septa, and internal blood flow. Additionally, US guided punctures and steroid injections into the ganglion are safe and efficient.
Pathological Findings of the Hand
Tenosynovitis of the flexor tendons
The typical ultrasound findings of tenosynovitis are: increased thickness of the tendon sheath due to its proliferation, increased amount of fluid within the sheath or both. The most impressive image of tenosynovitis is found in cases of dactylitis in patients with psoriatic arthritis. Dactylitis may affect any finger of the upper and/or lower limb.
If the thumb is involved, the US image depicts the flexor pollicis tendons surrounded by an anechoic or hypoechoic layer that corresponds to the inflamed proliferated synovial sheath and presence of fluid within it, (figure 8). It is always examined in two perpendicular planes. In cases of acute/subacute inflammatory conditions presence of Doppler signal may be occurred.
{kind=link}
Ganglia
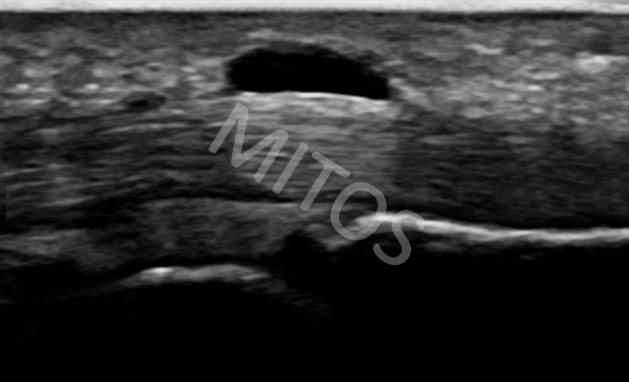
Ganglion is depicted as an aechoic, well-defined structure above the tendons, taking its origin from the annular ligaments – pulleys. The most common location of ganglion in this region is considered to be involvement of the A1 pulley, (figure 9).
{kind=link}
Pulley rupture
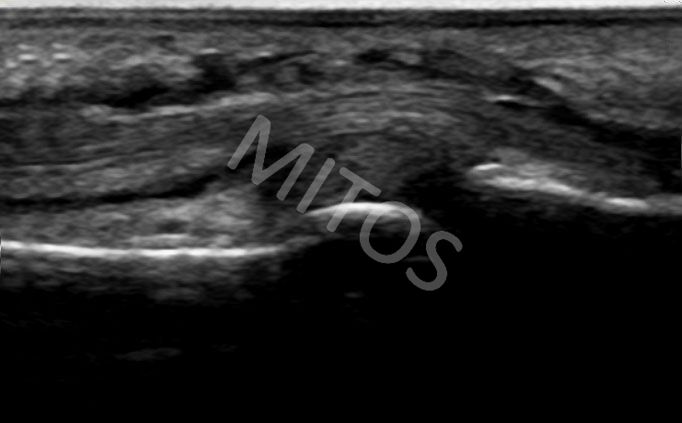
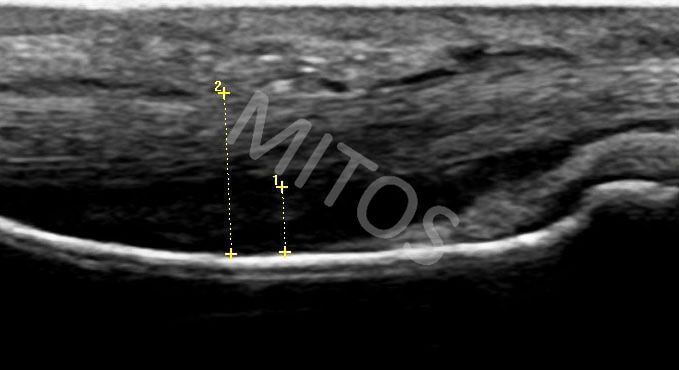
Pulley rupture is usually seen after intense manual effort, most commonly in the middle and ring fingers. In this case, an increased distance between the affected flexor tendon and the bony contour is found (indirect indication of the annular ligament rupture), (figure 10a). If Doppler mode is applied in this case, the presence of a signal is displayed within the inflicted area, (figure 10b).
{kind=link}
{kind=link}
Erosions
Erosions are visualized as a clear discontinuity of the bony contour. They are most frequently seen over the metacarpal heads. They may be single or multiple up to complete disorganization of the head. Often, hypoechoic content, corresponding to a synovial hypertrophy may be present within erosions, (figure 11a). Using the Doppler mode, active inflammation of both, synovitis and erosion can be detected, (figure 11b). The medial aspect of the 2nd MCP joint is the most common location to detect early erosions, well before they become apparent on plain radiography.
{kind=link}
{kind=link}
Crystal induced arthropathies
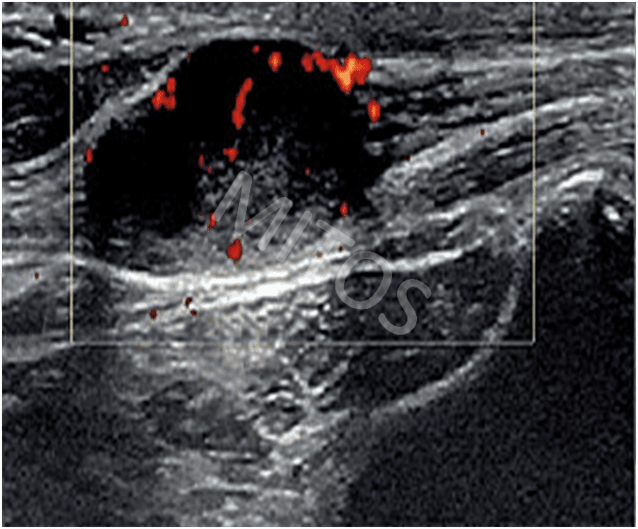
In a patient with chronic gout, a large mass of mixed echogenicity is sometimes seen near the clinically painful joint (usually the 2nd MCP) corresponding to a tophus. In case of inflammation, if Doppler mode is applied, a positive signal is found. In patients with chronic gout and longstanding hyperuricemia, the pathognomonic “double contour sign” is sometimes depicted, (figure 12).
{kind=link}
Osteoarthritis (OA)
The trapeziometacarpal joint at the base of the thumb as well as proximal and distal interphalangeal joints, are very common sites of OA. In OA, ultrasound can show both degenerative and inflammatory changes. Osteophytes are recognized as single or multiple characteristic “step-up” bone lesions of the bony margin at the ends of the articular surfaces, while narrowing of the interarticular space is also present, (figure 13a, figure 13b).
{kind=link}
{kind=link}
Bibliography:
- Filipucci E, Iagnocco A, Meenagh G et al. Ultrasound Imaging for the Rheumatologist. VII.Ultrasound Imaging in Rheumatoid Artrhritis. Clin Exp Rheum 2007;25:5-10.
- Hammer HB, Bolton-king P, Bakkeheim V et al. Examination of intra and interrater variability with a new ultrasonographic reference atlas for scoring of synovitis in patients with rheumatoid arthritis. Ann Rheum Dis 2011 Jul 22 (e-pub)
- Guttierez M, Filipucci E, Salaffi F et al. Differential diagnosis between rheumatoid arthritis and psoriatic arthritis:the value of ultrasonography at metacarpophalangeal joints level. Ann Rheum Dis 2011;70(6):1111-4.
- Machado PM, Koevoets R, Bombardier C. The value of magnetic resonance imaging and ultrasonography in undifferentiated arthritis: a systematic review. J Rheumatol (Suppl) 2011 Mar;87:31-7.
- Filer A, de Pablo P, Allen G et al. Utility of ultrasound ji=oint counts in patients with very early synovitis. Ann Rheum Dis 2011;70(3):500-7
- Backhaus M. Ultrasound and structural changes in inflammatory arthritis: synovitis and tenosynovitis. Ann N Y Acad Sci. 2009 Feb;1154:139-51. Review.
- Larché MJ, Seymour M, Lim A et al. Quantitative Power Doppler Ultrasonography Is a Sensitive Measure of Metacarpophalangeal Joint Synovial Vascularity in Rheumatoid Arthritis and Declines Significantly Following a 2-week Course of Oral Low-dose Corticosteroids. J Rheumatol. 2010 Oct 1.
- Naranjo A, Ojeda S, Araña V et al. Usefulness of clinical findings, nerve conduction studies and ultrasonography to predict response to surgical release in idiopathic carpal tunnel syndrome. Clin Exp Rheumatol. 2009 Sep-Oct;27(5):786-93.
- Dougados M, Jousse-Joulin S, Mistretta F et al. Evaluation of several ultrasonography scoring systems for synovitis and comparison to clinical examination: results from a prospective multicentre study of rheumatoid arthritis. Ann Rheum Dis. 2010 May;69(5):828-33.
- Scirè CA, Montecucco C, Codullo V et al. Ultrasonographic evaluation of joint involvement in early rheumatoid arthritis in clinical remission: power Doppler signal predicts short-term relapse. Rheumatology (Oxford). 2009 Sep;48(9):1092-7.
- Filippucci E, Meenagh G, Delle Sedie A et al. Ultrasound imaging for the rheumatologist. XX. Sonographic assessment of hand and wrist joint involvement in rheumatoid arthritis: comparison between two- and three-dimensional ultrasonography. Clin Exp Rheumatol. 2009 Mar-Apr;27(2):197-200.
- Meenagh G, Filippucci E, Delle Sedie et al. Ultrasound imaging for the rheumatologist. XVIII. Ultrasound measurements. Clin Exp Rheumatol. 2008 Nov-Dec;26(6):982-5.
- Rosenberg C, Etchepare F, Fautrel Bet al. Diagnosis of synovitis by ultrasonography in RA: a one-year experience is enough for reliability on static images. Joint Bone Spine. 2009 Jan;76(1):35-8.
- M. Szkudlarek, Ena Narvestad, M. Klarlund et al. Ultrasonography of the metatarsophalangeal joints in rheumatoid arthritis. Arthr Rheum 2004;50(7):2103-2112.