


KNEE
Giasna Giokits (Jasna Jokic)
The knee is one of the most commonly affected joints in inflammatory and non inflammatory rheumatic diseases. Due to various diseases that can affect it, and different clinical manifestations, imaging is mandatory to reach a diagnosis. Due to easy accessibility, ultrasound can provide multiple and valuable information about the knee pathology.
Pathologies detected with ultrasound
- Presence of even minimal amount of fluid within the joint cavity, joint recesses or bursae (superficial or deep), may be easily detected by US. They easily may be aspirated for diagnostic or therapeutic reasons.
- Presence of thickening or hypervascularization of the recesses and bursal walls,
- full or partial thickness tears of tendons and ligaments,
- lesions of bone or joint borderline (osteophytes, erosions) can be visualized, as well.
- Cartilage lesions: crystal deposits in hyaline and fibrocartilage and changes of cartilage thickness or echogenicity.
- Meniscal pathology (cysts or tears) can be seen by US. It should be taken into account that due to anatomical position of the menisci, ultrasound is unsuitable for their complete evaluation.
Synovitis
Synovial collection of fluid within the joint cavity, due to traumatic or inflammatory reasons, can easily be detected by ultrasound. Clinical examination can not reveal collections less than 6-8 ml, while plain X-rays are positive for the “fat pad separation sign”. “Fat pad separation sign“, detected by plain x-rays, is the presence of opacity between the two fat pads in case of presence of more than 5ml of synovial fluid.
For the proper US evaluation the patient is positioned in supine position with the knee flexed in 30-40%. By this approach even minimal amount of synovial fluid (1 ml) can be detected.
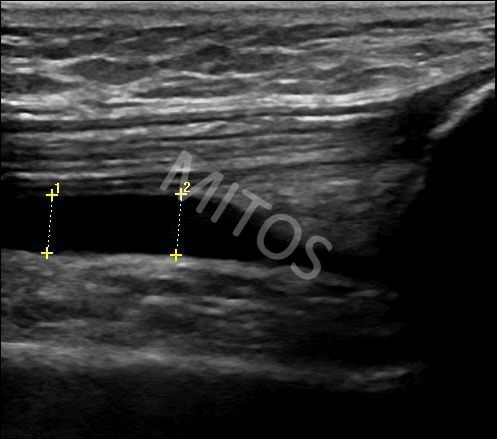
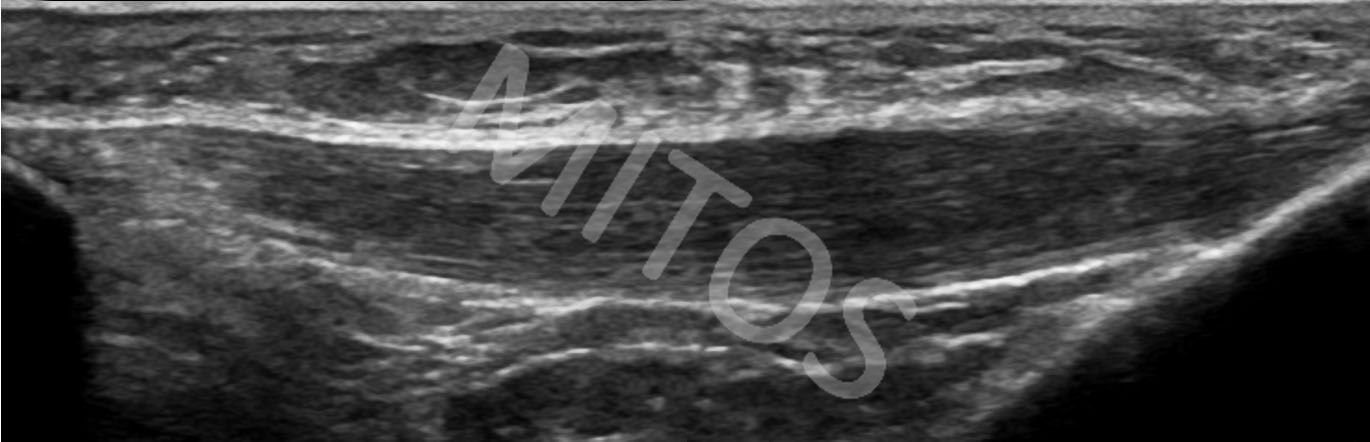
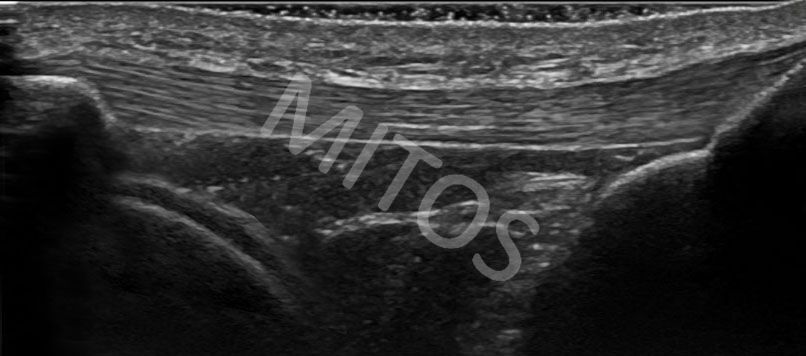
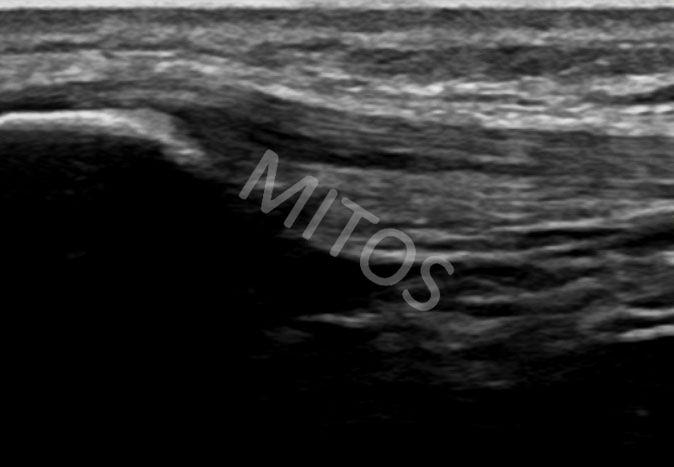
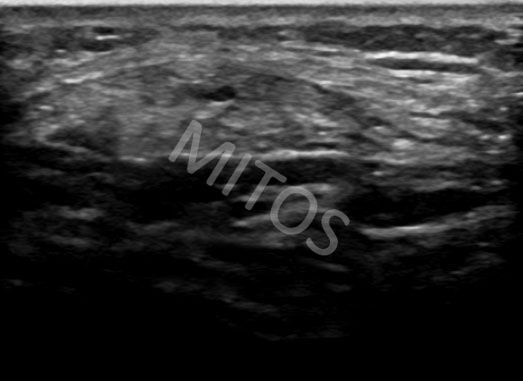
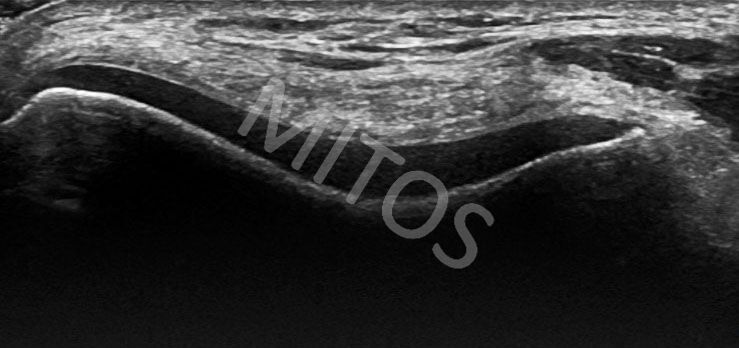
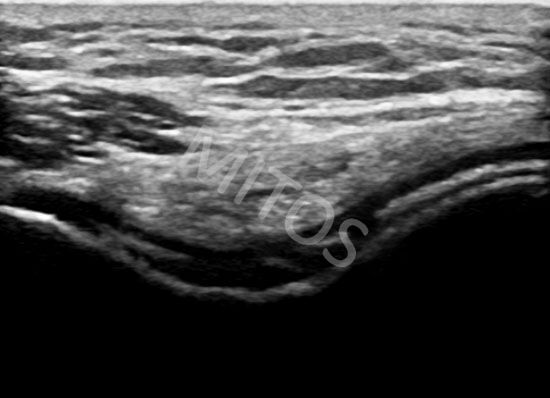
Patients with any kind of arthritis, may present different amount of fluid within the suprapatellar recess, (figure 1), presented on US image as a hypo or anechoic area. The fat pads are separated by fluid pressure and this image should be compared with the normal image, (figure 2).
{kind=link}
{kind=link}
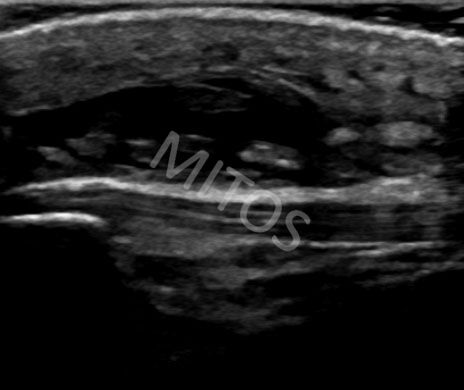
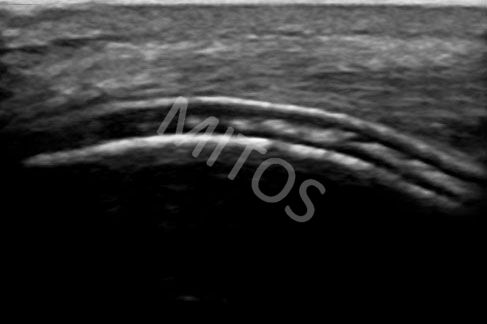
Performing dynamic examination, with the knee in extension and quadriceps muscle in contraction, even minimal amount of fluid within the suprapatellar recess can be depicted, (figure 3a).
{kind=link}
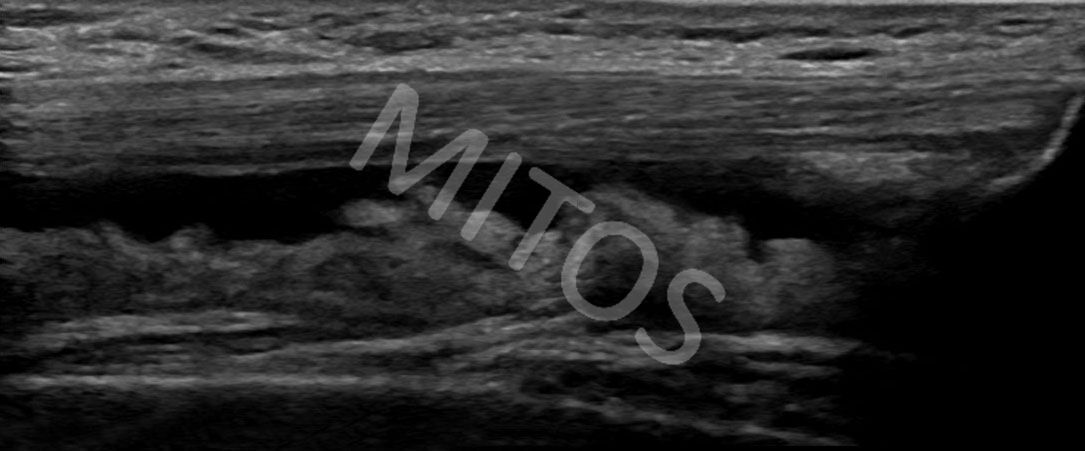
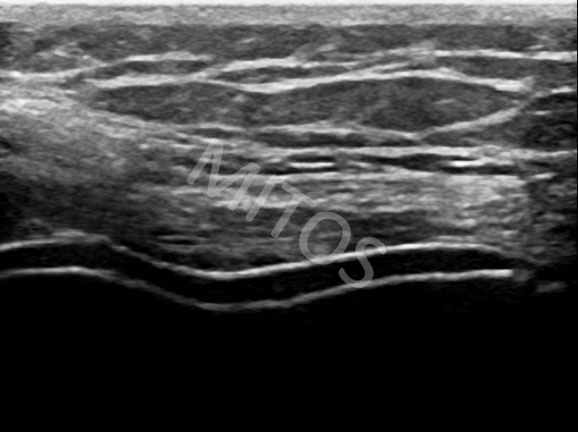
Additionally to presence of fluid, in cases of chronic inflammatory arthritis, synovial hypertrophy is frequently visualized, (figure 3b).
{kind=link}
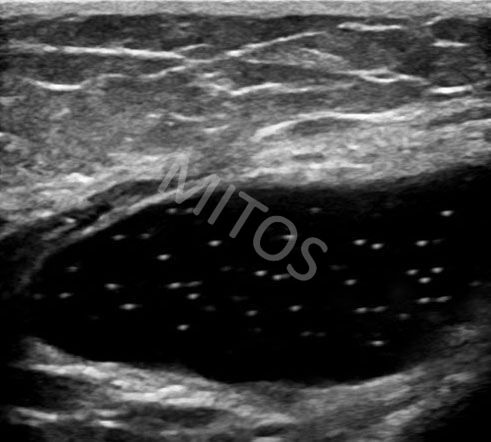
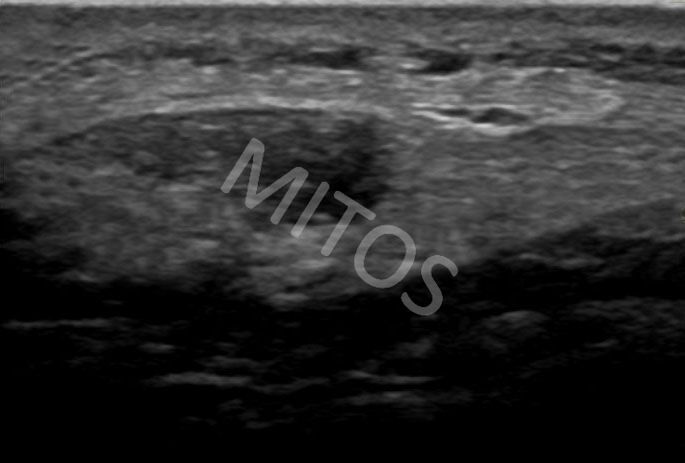
Presence of floating hyperechoic particles within the joint cavity could be considered as pathognomonic to gout, (figure 4).
{kind=link}
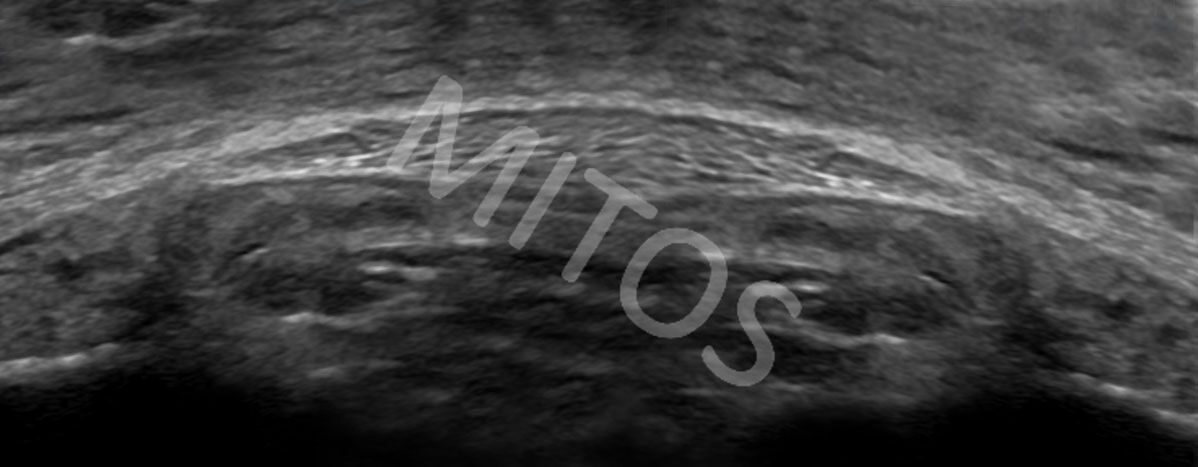
Any kind of synovitis can be accompanied by presence of a foreign body, which appears in a view of a hyperechoic structure, (figure 5a). This finding should be evaluated in two planes (both, in the long and the short scan) in order to define the exact position and the size of the structure, (figure 5b).
{kind=link}
{kind=link}
Pathology of the patellar tendon
The patellar tendon can be affected due to inflammatory or mechanical reasons.
Often, after prolonged kneeling due to the vocational reasons, patients appear with severe pain below the kneecap with a clinically slightly warm and swollen corresponding area. In this case, depicted by US, the patellar tendon can be thickened, hypoechoic and structurally disorganized due to severe inflammation, (figure 6a), compared to the normal ultrasound image, (figure 6b).
{kind=link}
{kind=link}
Athletes often present with similar clinical symptoms. The cranial pole of the patellar tendon is sometimes found swollen and of varying echogenicity (Jumper’s knee), (figure 7a), seen in both long and short scans, (figure 7b), compared to the normal image, (figure 7c). The presence of hypo-anechoic areas within the cranial pole of the patellar tendon, may indicate a partial thickness tear (figure 8a) in longitudinal and transverse planes, (figure 8b).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Careful examination of the lower part of the tendon is important even in asymptomatic patients. Osgood-Schlatter disease is a result of chronic repetitive tension of the apophyseal cartilage and the growth plate due to tendon traction. Progressively it guides to fragmentation of the tibial tuberosity and presence of calcification of the patellar tendon’s lower pole, (figure 9).
{kind=link}
The prepatellar bursa overlies the patellar tip and the patellar tendon’s upper pole. Ultrasound, in the case of inflammation, may reveal the area of mixed echogenicity, mainly anechoic, which corresponds to the subacute or chronically inflamed prepatellar bursa with a presence of fluid within it, (figure 10a) – “housemaid’s knee”.
{kind=link}
The lower pole of the patellar tendon may show a similar ultrasound image. The superficial infrapatellar bursa overlies the distal pole of the patellar tendon and the upper part of the tibial tubercle. In case of inflammation, an area of mixed echogenicity, mostly anechoic (due to the presence of fluid) is found, which corresponds to the inflamed superficial infrapatellar bursa, (figure 10b).
{kind=link}
Pathology of the medial part of the knee
Abnormalities of the bony outline (femoral and tibial condyle), pathology of the medial meniscus base and of the medial collateral ligament can be obtained by US.
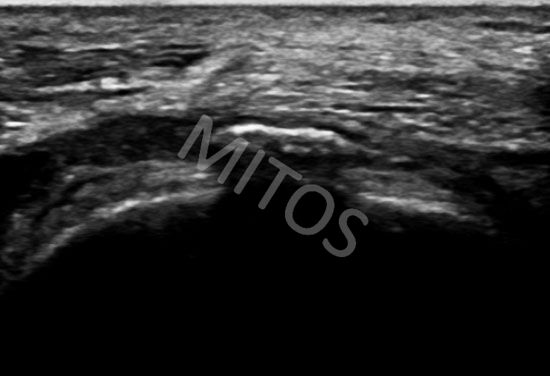
In the typical ultrasound image of Osteoarthritis, the presence of osteophytes of both condyles (cranial of the femoral and caudal of the tibial condyle) is depicted. They are usually accompanied with the medial meniscus of deranged echogenicity, protruding outside the joint limits, (figure 11a).
{kind=link}
The medial collateral ligament is usually displaced medially, in comparison to the normal ultrasound image, (figure 11b). An anechoic zone that separates the superficial from the deep medial collateral ligament layers is a characteristic finding of inflammation of the medial collateral ligament bursa (bursitis). It can be found in inflammatory, degenerative or post-traumatic cases, (figure 11c). Comparative to the normal ultrasound image (figure 11b).
{kind=link}
{kind=link}
Pathology of the femoral trochlea
For the proper evaluation of the femoral trochlea, a patient is in supine position with the knees in maximum possible flexion. The most common findings are changes of thickenss and/or echogenicity of the trochlear cartilage.
The trochlear cartilage of reduced thickens and more echogenic appearance, as well as lesions of the cartilage-bone interface are usually seen in Osteoarthritis.
In cases of chronic gout it is possible to detect (while the knee in the same position), two parallel hyperechoic lines, that are highly supportive of gout (double contour sign), (figure 12a), compared to normal findings, (figure 12b).
{kind=link}
{kind=link}
In patients who suffer from chronic pyrophosphate arthropathy (CCPD), focal or multiple echogenic foci within the cartilage, potentially pathognomonic for calcium pyrophosphate deposition are visualized, (figure 12c, figure 12d).
{kind=link}
{kind=link}
Baker cyst
Baker cyst imaging was the first attempt to apply ultrasound in Rheumatology and the musculoskeletal diseases. In acute or subacute conditions, a typical ultrasound image of an anechoic “cloud”- shaped structure in between the semimembranosus and gastrocnemius tendons corresponds to a Baker’s cyst, (figure 13a), compared to a normal ultrasound image of the region, (figure 13b).
{kind=link}
{kind=link}
In chronic cases, Baker’s cyst is typically presented with thickened walls, (figure 13c).
{kind=link}
Bibliography:
- GAW Bruyn and WA Schmidt, “Introductory Guide to Musculoskeletal Ultrasound for the Rheumatologist”, Bon Stafleu van Loghum, the Netherlands, 2006.
- Bianchi, C. Martinoli, “Ultrasound of the Musculoskeletal System”, Springer-Verlag, Berlin, 2007.
- Backhaus M, Burmester G-R, Gerber T et al. Guidelines for Musculoskeletal Ultrasound in Rheumatology. Ann Rheum Dis 2001;60:641-649.
- Backhaus M. Ultrasound and structural changes in inflammatory arthritis: synovitis and tenosynovitis. Ann N Y Acad Sci. 2009 Feb;1154:139-51. Review.
- Filipucci E, Iagnocco A, Meenagh G et al. Ultrasound Imaging for the Rheumatologist. VII.Ultrasound Imaging in Rheumatoid Artrhritis. Clin Exp Rheum 2007;25:5-10.
- Filer A, de Pablo P, Allen G et al. Utility of ultrasound joint counts in patients with very early synovitis. Ann Rheum Dis 2011;70(3):500-7
- Carpenter JR, Hattery RR, Hunder GG, Bryan RS, McLeod RA. Ultrasound evaluation of the popliteal space. Comparison with arthrography and physical examination. Mayo Clin Proc 1976;51: 498–503.
- Kane D, Balint PV, Sturrock RD. Ultrasonography is superior to clinical examination in the detection and localization of knee joint effusion in rheumatoid arthritis. J Rheumatol 2003;30:966–71.
- Grassi W, Meenagh G,. Pascual E, Filippucci E. “Crystal Clear”—Sonographic Assessment of Gout and Calcium Pyrophosphate Deposition Disease. Semin Arthritis Rheum 2006;36:197-202
- Frediani B, Filippou G, Falsetti P, Lorenzini S, Baldi F, Acciai C, et al. Diagnosis of calcium pyrophosphate dihydrate crystal deposition disease: ultrasonographic criteria proposed. Ann Rheum Dis 2005;64:638-40.
- Grassi W, Filippucci E, Farina A, Cervini C. Sonographic imaging of tendons. Arthritis Rheum 2000;43:969–76.
- Campbell RS, Grainger AJ. Current concepts in imaging of tendinopathy. Clin Radiol 2001;56:253–67.
- Scirè CA, Montecucco C, Codullo V et al. Ultrasonographic evaluation of joint involvement in early rheumatoid arthritis in clinical remission: power Doppler signal predicts short-term relapse. Rheumatology (Oxford). 2009 Sep;48(9):1092-7.
- Meenagh G, Filippucci E, Delle Sedie et al. Ultrasound imaging for the rheumatologist. XVIII. Ultrasound measurements. Clin Exp Rheumatol. 2008 Nov-Dec;26(6):982-5.