


ANKLE JOINT
Giasna Giokits (Jasna Jokic)
The ankle joint as well as the foot displays an extremely complex anatomical structure. Considering the various pathology of the area (of the joints, synovial cavities and synovial sheaths), the ultrasound (US) method became particularly useful method for the diagnosis and therapeutic management of this region.
According to the EULAR guidelines, there are eight standard scans that allow full evaluation of the ankle joint and additional six scans for the full evaluation of the foot.
For the proper evaluation, the patient is positioned in a supine position with the knee flexed 50-60° while the foot is in mild plantar flexion laying on the examination bed.
A high frequency transducer (10-15 MHz) is used.
Synovitis of the ankle joint
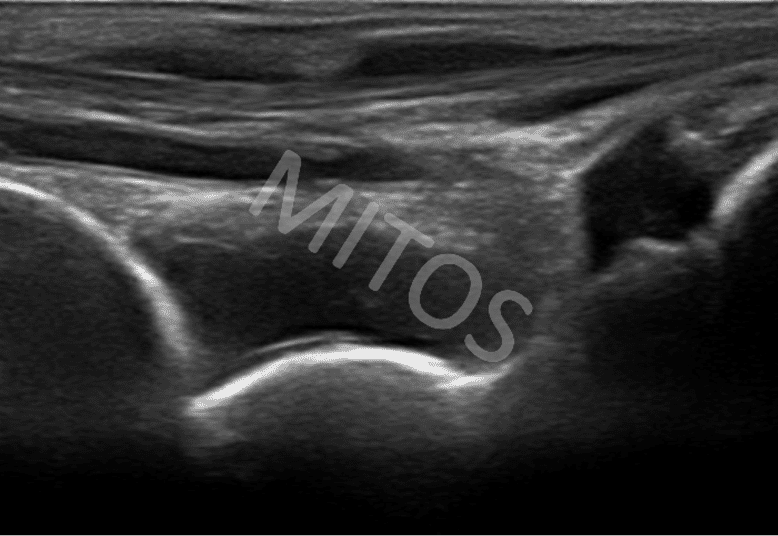
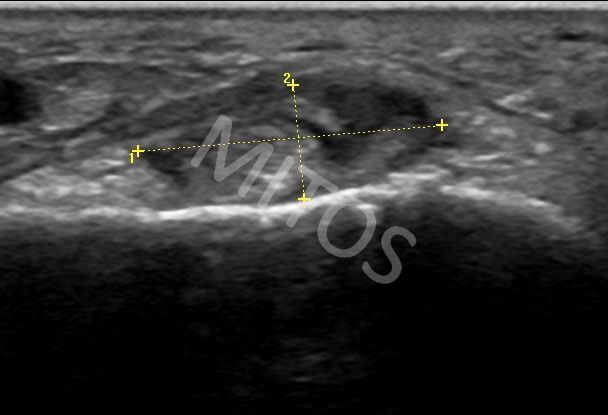
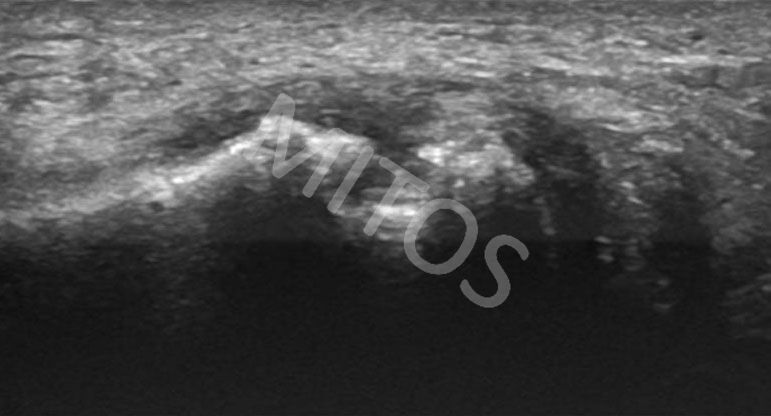
The most frequent pathological finding, regardless of its cause, in the region of the ankle joint, is undoubtedly the collection of fluid within it. In patients with a clinically swollen, warm and painful area of the ankle joint, on ultrasound examination the fat pad is displaced upwardly, due to the “pressure” of the anechoic collection of fluid within the synovial cavity.
It is more often found unilaterally in patients with inflammatory spondyloarthropathies, (figure 1).
{kind=link}
In patients with rheumatoid arthritis, synovitis is usually occurred bilaterally.
Pathology of the tarsal tunnel
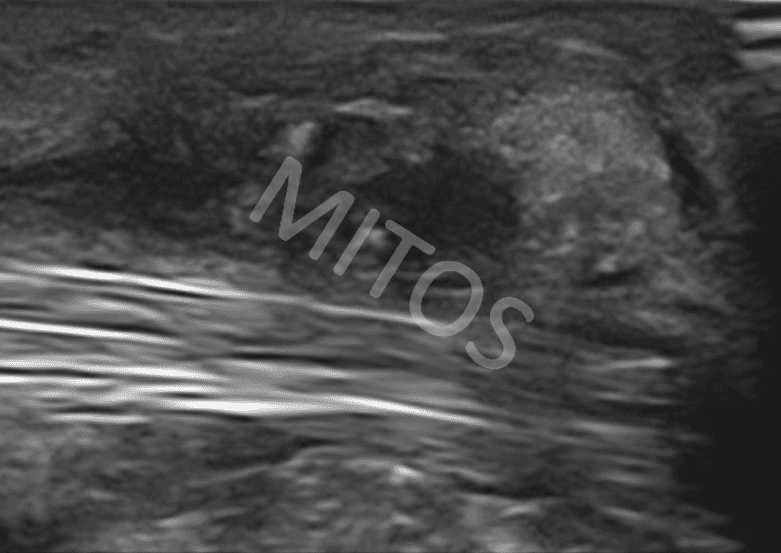
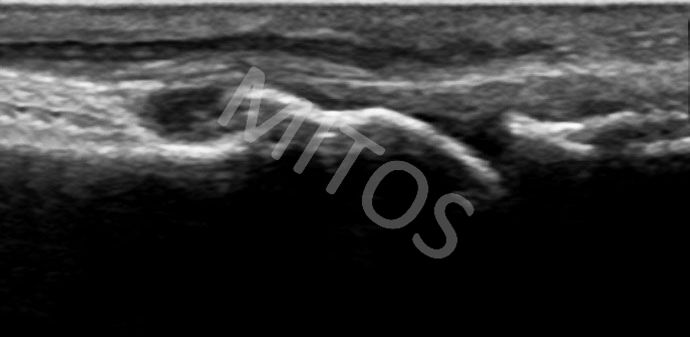
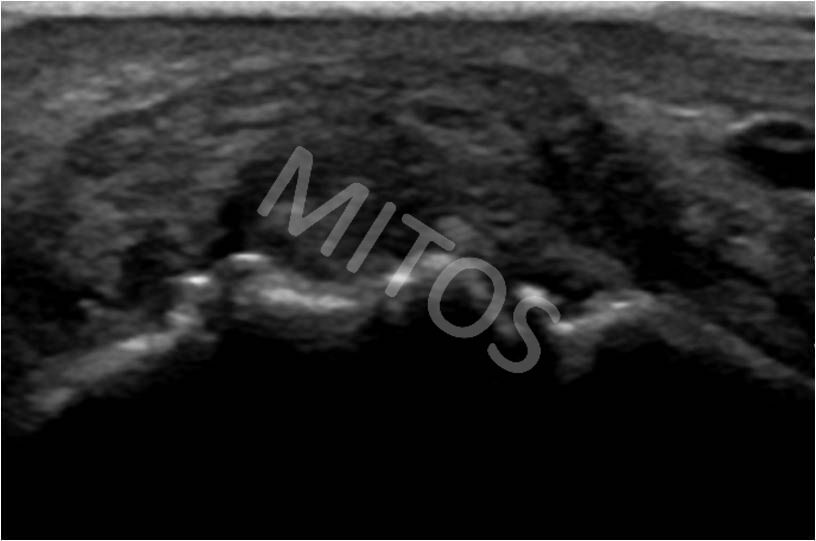
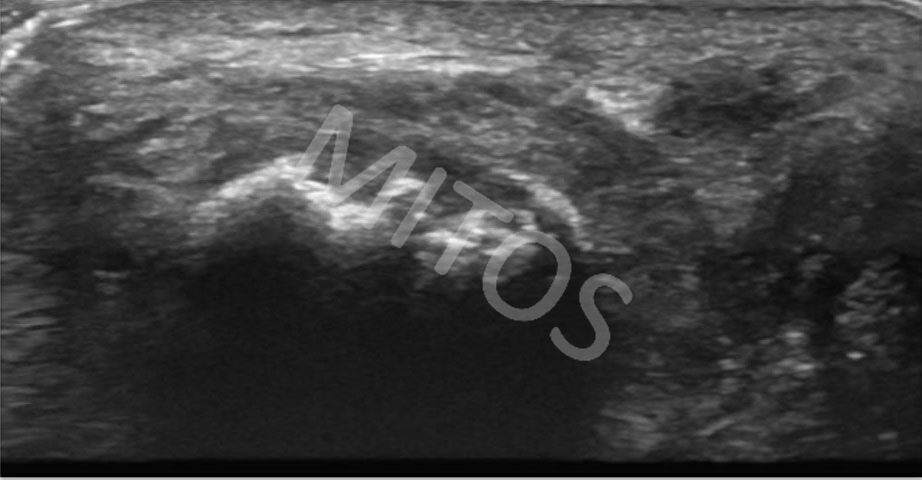
Pathology of the tarsal tunnel is frequently found in inflammatory, degenerative, vascular or post-traumatic lesions. In a clinically swollen, warm, and painful area of the ankle joint, additionally to a mild collection of fluid within the joint, US may also demonstrate severe enlargement and inflammation of the tendons and tendon sheaths within the tarsal tunnel.
The tendons of the posterior tibial and the long flexor digitorum muscles are most commonly affected, (figure 2a, figure 2b). In the case of inflammation and the presence of fluid within the synovial sheath, they should be checked in both ultrasound planes (long and the short).
{kind=link}
{kind=link}
Pathology of the peroneal tendons
All the tendons in the region of the ankle joints are frequently affected by various pathological causes (inflammatory, degenerative or post-traumatic).
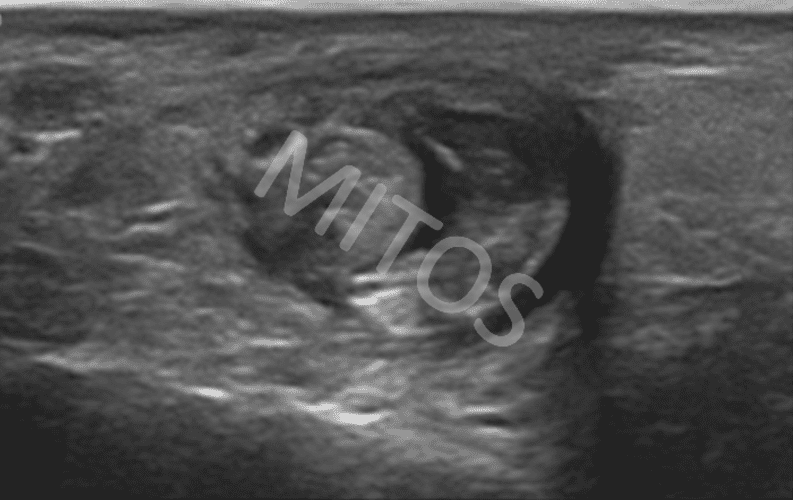
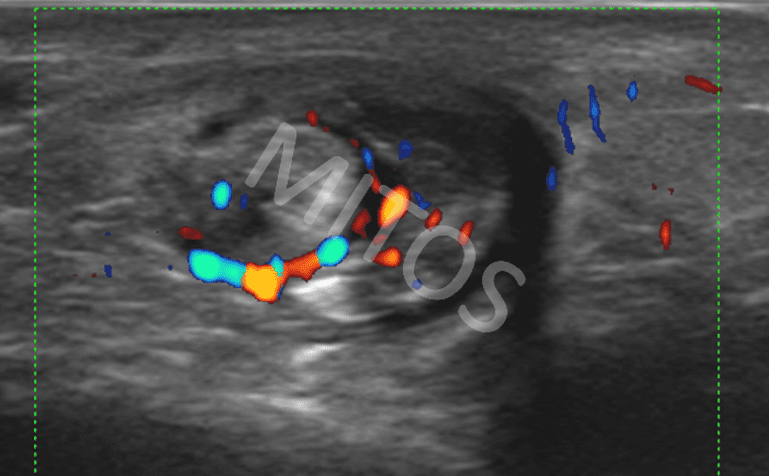
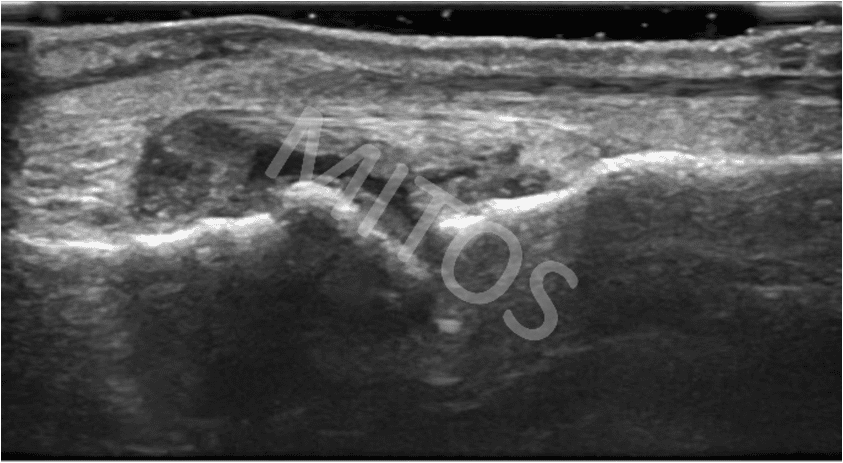
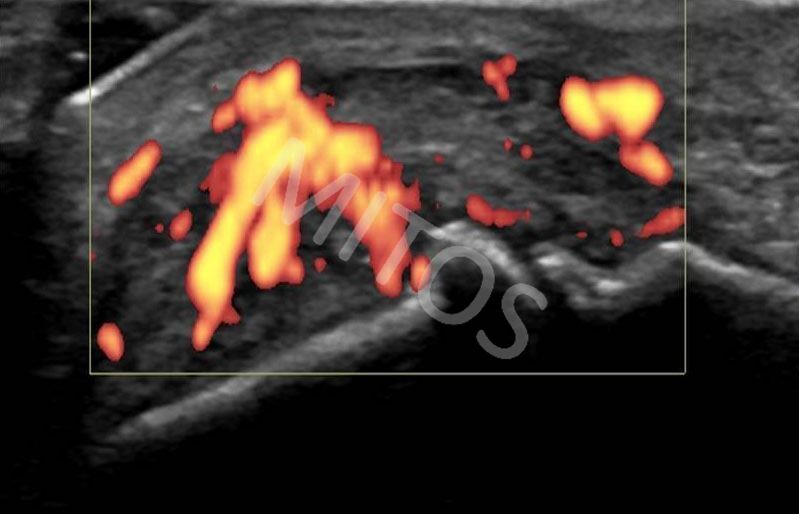
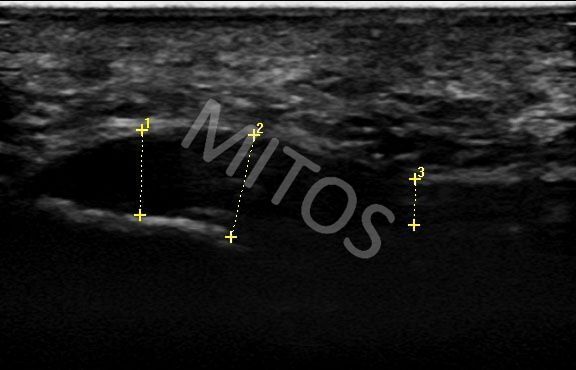
Post-traumatically, the peroneal tendons are frequently present with tenosynovitis, usually unilateral, in association with fluid collection within the ankle joint, (figure 3a, figure 3b). The same structure is checked in both ultrasound plans while using the Doppler mode, (figure 3c).
{kind=link}
{kind=link}
{kind=link}
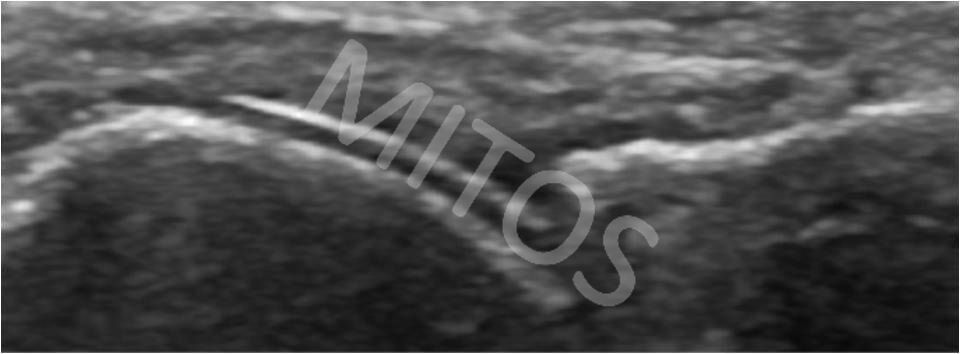
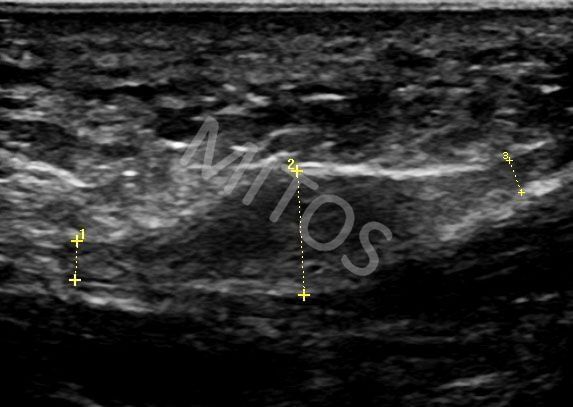
In the case of patient, whose both peroneal tendons are affected, (depicted in long scan), posteriorly to the lateral malleolar tip, the peroneal tendons split, while each of the tendon is surrounded by a presence of fluid within its sheath.
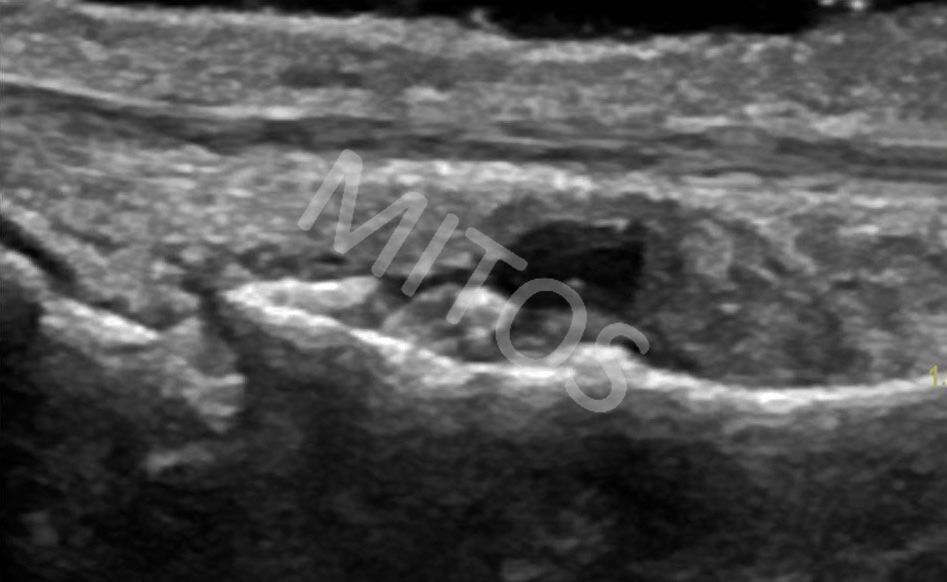
A similar ultrasound image is found in patients with early RA, (figure 4a, figure 4b).
{kind=link}
{kind=link}
In case of a chronic inflammation, of any etiology, the ultrasound image is different.
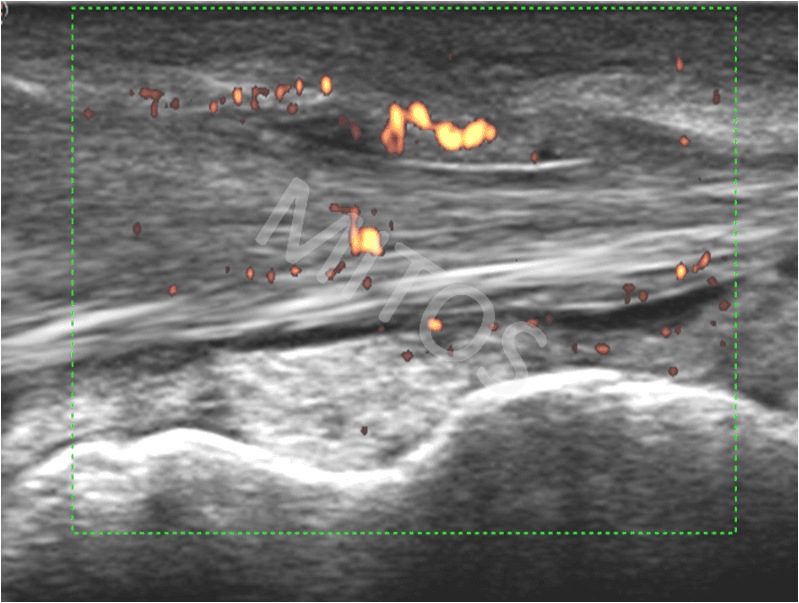
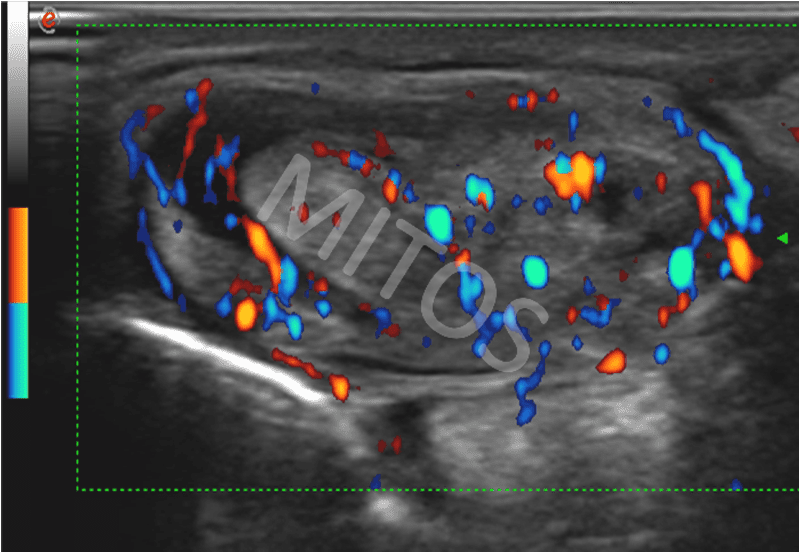
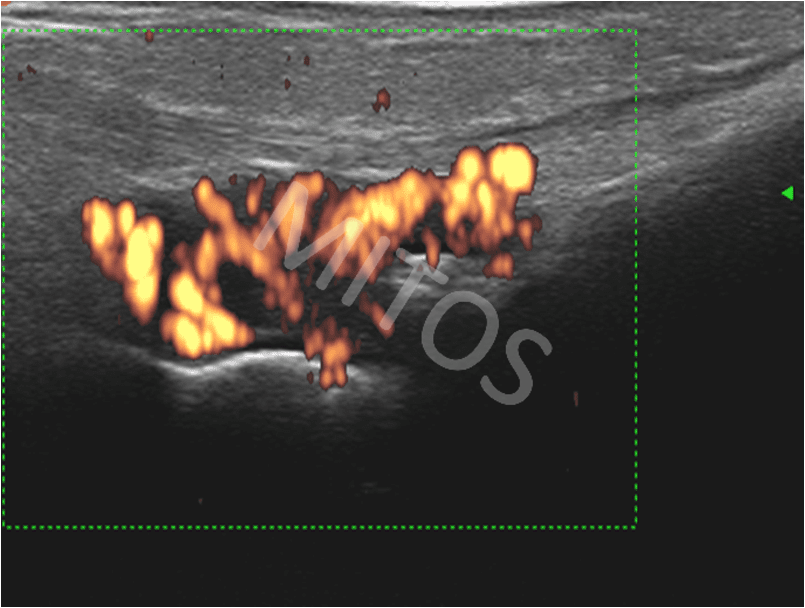
The borderline and the content of the peroneal tunnel in a patient with e.g. psoriatic arthritis is seriously disorganized. The tendons are depicted as structures of mixed echogenicity, due to chronic inflammation. Additionally, they are surrounded by the hypertrophic sheaths of mixed echogenicity, (figure 5a, figure 5b). The presence of Doppler signal, both within the sheath and within the tendons, is frequently found in such cases, (figure 5c, figure 5d).
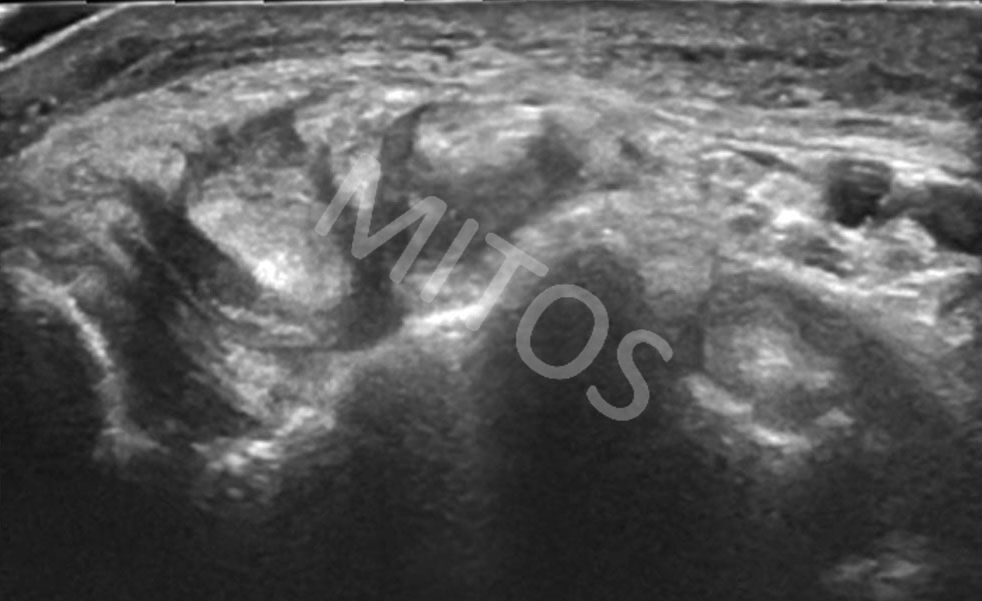{kind=link}
{kind=link}
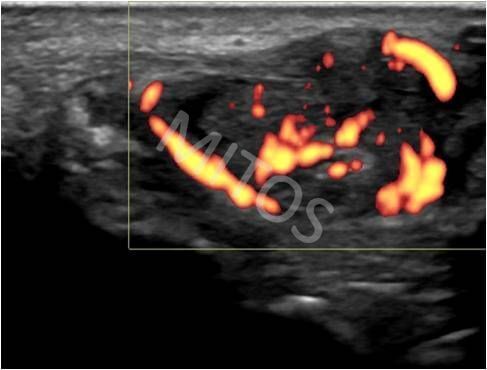{kind=link}
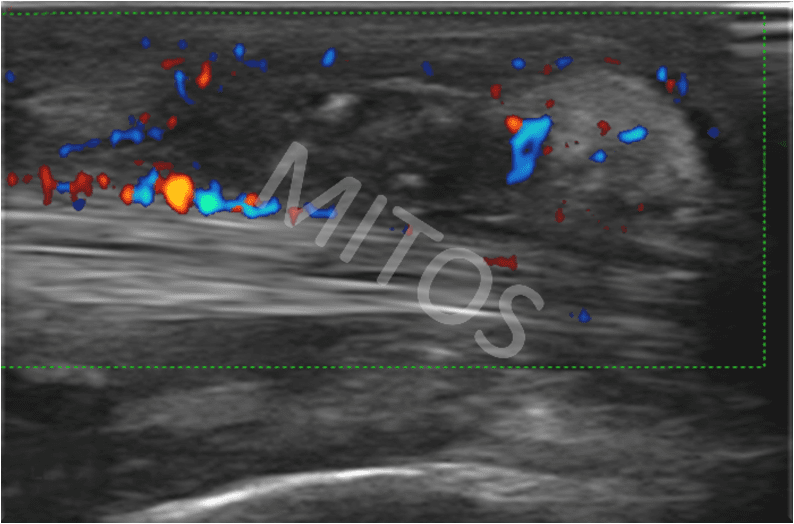{kind=link}
Pathology of the Achilles tendon
Pathological findings of the Achilles tendon are extremely common in patients with inflammatory, post-traumatic and degenerative conditions. The mid-third part of the tendon is most frequently affected. Sonographically, an enlargement of this part of the tendon is seen, while the tendon itself is depicted as mainly hypoechoic and with seriously disorganized ultrasound echotexture.
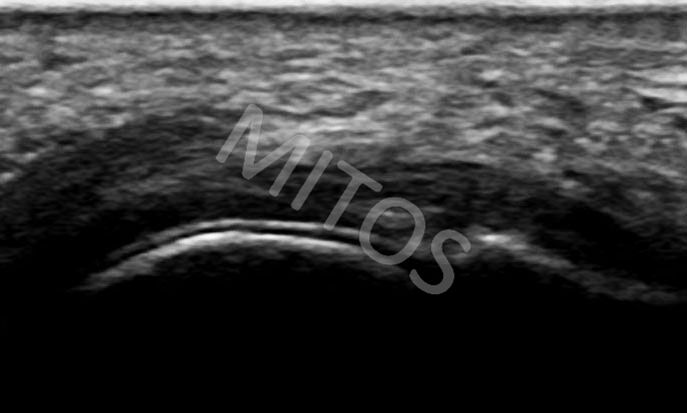
In the case of inflammation of the retrocalcaneal bursa, the anechoic area of fluid collection can be visualized along with bony erosions underneath, (figure 6a).
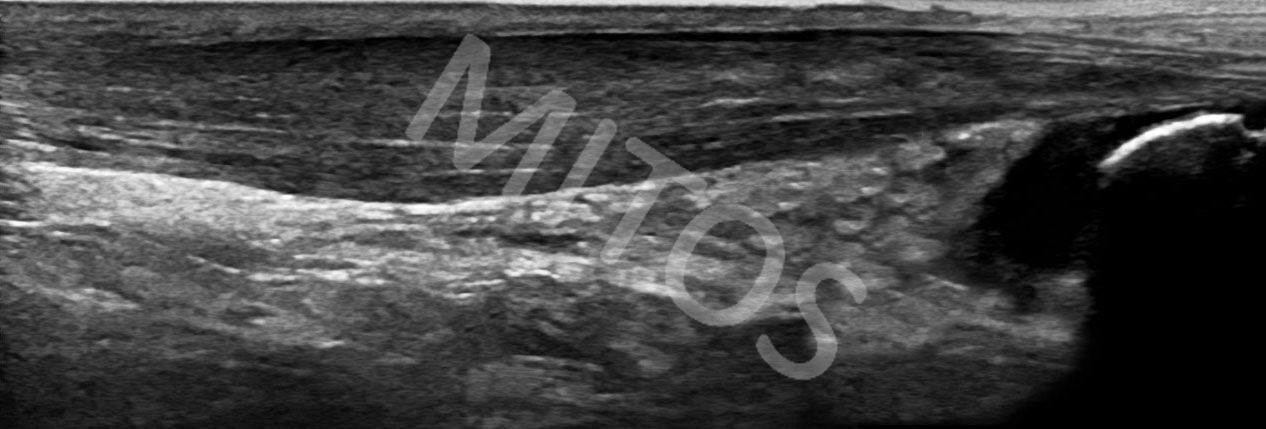{kind=link}
Presence of Doppler signal in the region of the inflamed retrocalcaneal bursa and adjacent tendons can determine the severity of the inflammatory lesion, (figure 6b).
{kind=link}
In patients with the Achilles tendon chronic inflammation of any etiology, while the posterior long scan is applied, an enlarged Achilles tendon of mixed echogenicity is found, (figure 7). Sometimes echogenic foci due to calcifications presence may be seen.
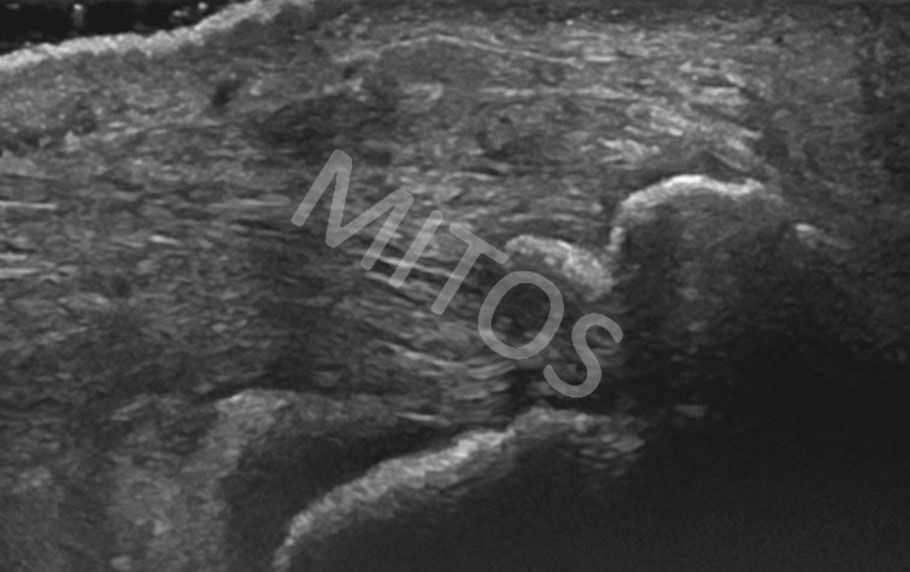{kind=link}
Bibliography:
- Bruyn GAW , Schmidt WA. Introductory Guide to Musculoskeletal Ultrasound for the Rheumatologist, Bon Stafleu van Loghum, the Netherlands, 2006.
- Bianchi S, Martinoli C. Ultrasound of the Musculoskeletal System, Springer-Verlag, Berlin, 2007.
- Backhaus M, Burmester G-R, Gerber T et al. Guidelines for Musculoskeletal Ultrasound in Rheumatology. Ann Rheum Dis 2001;60:641-649.
- Wakefield J.R, D’Agostino MA. Essential applications of Musculoskeletal Ultrasound in Rheumatology, Saunders Elsevier, Philadelphia,
- Holsbeeck T.M, Introcaso H.J. Musculoskeletal Ultrasound, Mosby of Elsevier, St Louis, Missouri, 2001.
- Filipucci E, Iagnocco A, Meenagh G et al. Ultrasound Imaging for the Rheumatologist. VII.Ultrasound Imaging in Rheumatoid Artrhritis. Clin Exp Rheum 2007;25:5-10.
- Balint PV, Kane D, Wilson H, McInnes IB, Sturrock RD. Ultrasonography of entheseal insertions in the lower limb in spondyloarthropathy. Ann Rheum Dis 2002;61:905–10.
- D’Agostino MA, Said-Nahal R, Hacquard-Bouder C, Brasseur JL, Dougados M, Breban M. Assessment of peripheral enthesitis in the spondylarthropathies by ultrasonography combined with power Doppler: a cross-sectional study. Arthritis Rheum 2003;48:523–33.
- McGonagle D, Marzo-Ortega H, O’Connor P et al. Histological assessment of the early enthesitis lesion in spondyloarthropathy. Ann Rheum Dis 2002;61:534–7.
- Nazarian LN, Rawool NM, Martin CE, Schweitzer ME. Synovial fluid in the hindfoot and ankle: detection of amount and distribution with US. Radiology 1995;197:275–8.
- Filer A, de Pablo P, Allen G et al. Utility of ultrasound joint counts in patients with very early synovitis. Ann Rheum Dis 2011;70(3):500-7
- Backhaus M. Ultrasound and structural changes in inflammatory arthritis – synovitis and tenosynovitis. Ann N Y Acad Sci. 2009 Feb;1154:139-51. Review.
- Hau M, Schultz H, Tony HP et al. Evaluation of pannus and vascularization of the metacarpophalangeal and proximal interphalangeal joints in rheumatoid arthritis by high-resolution ultrasound (multidimensional linear array). Arthritis Rheum 1999; 42:2303–8.
- Martinoli C, Bianchi S, Derchi LE. Tendon and nerve sonography. Radiol Clin North Am 1999;37:691–711, viii.
- Fornage BD. The case for ultrasound of muscles and tendons. Semin Musculoskelet Radiol 2000;4:375–91.
- Dougados M, Jousse-Joulin S, Mistretta F et al. Evaluation of several ultrasonography scoring systems for synovitis and comparison to clinical examination: results from a prospective multicentre study of rheumatoid arthritis. Ann Rheum Dis. 2010 May;69(5):828-33.
- Gerster JC, Landry M, Dufresne L, Meuwly JY. Imaging of tophaceous gout: computed tomography provides specific images compared with magnetic resonance imaging and ultrasonography. Ann Rheum Dis 2002;61:52-4.
- Grassi W, Meenagh G,. Pascual E, Filippucci E. “Crystal Clear”—Sonographic Assessment of Gout and Calcium Pyrophosphate Deposition Disease. Semin Arthritis Rheum 2006;36:197-202
- Frediani B, Filippou G, Falsetti P, Lorenzini S, Baldi F, Acciai C, et al. Diagnosis of calcium pyrophosphate dihydrate crystal deposition disease: ultrasonographic criteria proposed. Ann Rheum Dis 2005;64:638-40.
- Scirè CA, Montecucco C, Codullo V et al. Ultrasonographic evaluation of joint involvement in early rheumatoid arthritis in clinical remission: power Doppler signal predicts short-term relapse. Rheumatology (Oxford). 2009 Sep;48(9):1092-7.
- Meenagh G, Filippucci E, Delle Sedie et al. Ultrasound imaging for the rheumatologist. XVIII. Ultrasound measurements. Clin Exp Rheumatol. 2008 Nov-Dec;26(6):982-5.
- Rosenberg C, Etchepare F, Fautrel Bet al. Diagnosis of synovitis by ultrasonography in RA: a one-year experience is enough for reliability on static images. Joint Bone Spine. 2009 Jan;76(1):35-8.
FOOT
Giasna Giokits (Jasna Jokic)
According to the EULAR guidelines, six standard scans are used for the full investigation of the foot. To perform the first three scans, the patient is in a supine position with the knee flexed in 50-60° and the foot in slight dorsal extension lying on the examination bed. A high frequency transducer (10-15 MHz) is used.
Pathology of the metatarsophalangeal and intermetatarsal joints is found typically in elderly patients, especially in patients with flat feet and hallux valgus.
In case of tendinopathy of the anterior tibial tendon, it is depicted as enlarged with mainly hypoechoic appearance, (figure 1a). The anterior tibial tendon overlies the scaphoid and medial cuneiform bone. It is stabilized by the superior and inferior extensor retinacula. On its transverse scan, (figure 1b), below the inferior extensor retinaculum, the tibialis anterior tendon is presents as enlarged and of mixed echogenicity, due to disorganization of its fibrillar structure (tendinopathy).
{kind=link}
{kind=link}
Synovitis
The 1st metatarsophalangeal (MTP) joint is the most frequently affected MTP joint in OA, inflammatory and crystal induced arthritides. In patients with hallux valgus and/or flat feet, US can detect rough osteophytes protruding from the articular edge of the metatarsal head, (figure 2).
{kind=link}
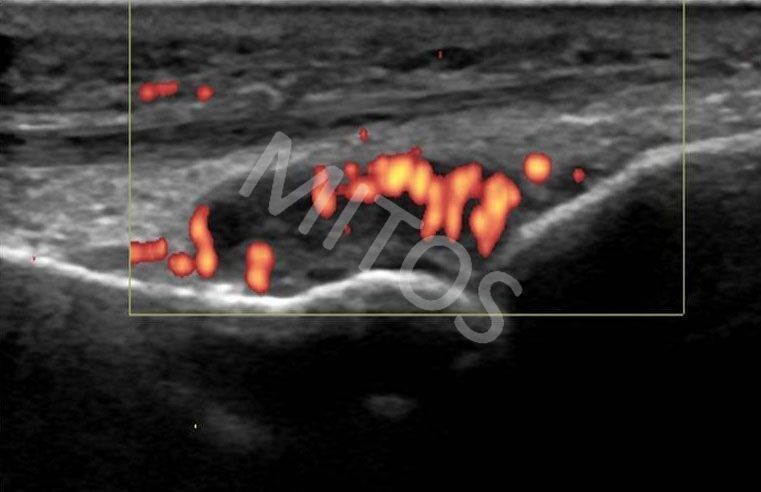
In patients with inflammatory arthropathy, additionally to the presence of fluid within the synovial cavity and synovial hypertrophy (figure 3a, figure 3b), the Doppler signal may be seen within the synovial layer, (figure 3c). These finding should be visualized in both ultrasound planes, short and long.
{kind=link}
{kind=link}
{kind=link}
Crystal induced arthritides
Some US findings such as the double contour, snowstorm, and starry night sign are considered to be strongly supportive for the diagnosis of gout. In addition to the personal and family history, the patient’s clinical image and blood tests, these findings enhance the diagnosis of gout.
Often in patients with known and long-term gout, a lesion of variable echogenicity is found in close proximity to the 1st MTP joint, that corresponds to tophi, (figure 4).
{kind=link}
US findings in patients with a gout flare differ from findings chronic gout.
Acute gout
In acute gout the US image of the inflamed 1st MTP joint does not differ significantly from its imaging in other inflammatory arthritides in both, either B mode or Doppler mode, (figure 5a, figure 5b).
{kind=link}
{kind=link}
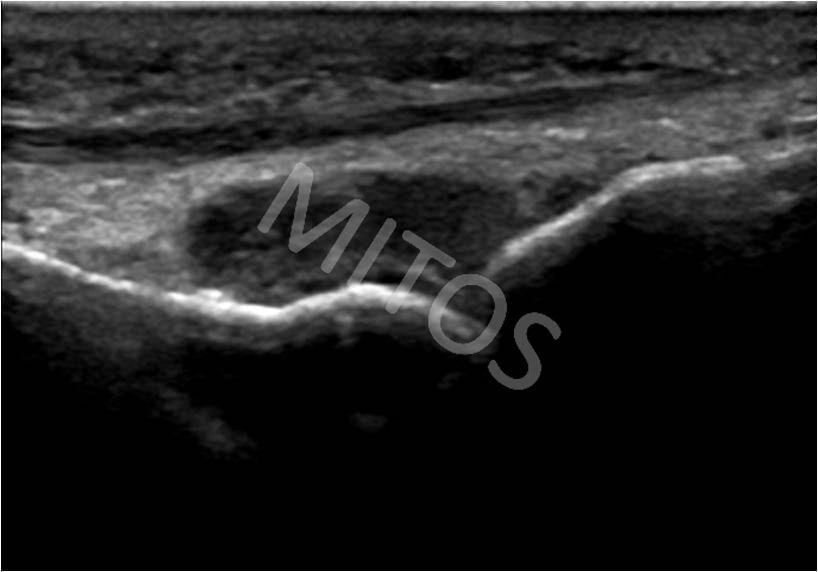
In contrast, in a patient with a chronic disease flare, alongside the eroded bony contour of the 1st metatarsal head and the base of the proximal phalanx (figure 6a) may be found a mass of mixed echogenicity without acoustic shadow that corresponds to the image of “soft” tophus, (figure 6b). In these cases, the presence of a Doppler signal is noted in the area in question, (figure 6c).
{kind=link}
{kind=link}
{kind=link}
Chronic gout
The double contour sign can also be found in the small joints, usually in the 1st, 2nd and 3rd MTF joints, (figure 7a, figure 7b).
{kind=link}
{kind=link}
Erosions
Undoubtedly, the most important advantage of US application in inflammatory arthritides is finding, recording and monitoring of erosions. The earliest and at the same time most frequent point of erosions’ occurrence is the 5th MTP joint, specifically the head of the 5th metatarsal bone, (figure 8a). This finding is verified on both sonographic planes, (figure 8b).
{kind=link}
{kind=link}
At the same time, in a patient with RA, apart from erosions, an enlarged, mostly hypoechoic soft tissue lesion that overlies the joint itself may be found. It corresponds to the inflamed and hypertrophied synovial membrane, (figure 9).
{kind=link}
Pathology of the plantar aponeurosis
Plantar fasciitis is the most common cause of heel pain. The pathology of this area is more frequently found in elderly and obese people as well as in people with intense physical fatigue. Due to histological, anatomical, topographical and mechanical peculiarities of this area, heel pain should be carefully evaluated. Frequently, and especially in younger people it may be caused by enthesopathy, found in the context of Seronegative Spondyloarthropathy.
A small percentage of patients can develop plantar fasciitis as part of other systemic diseases such as RA and gout. An increased incidence has also been observed in patients with Achilles tendon pathology.
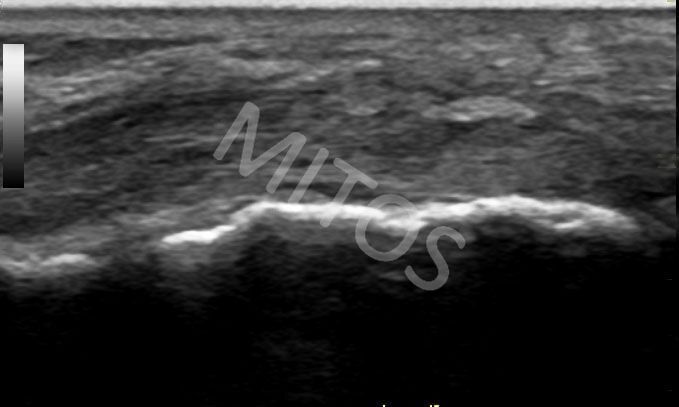
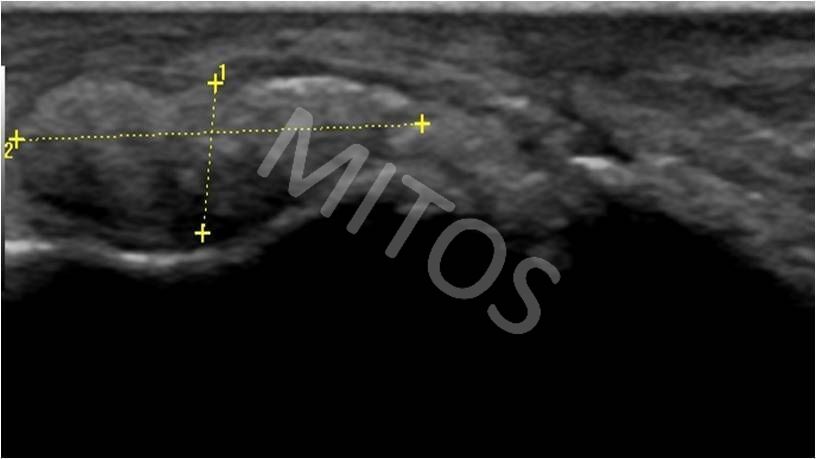
Clinical image of heel pain varies. In patients with calcaneal spur, continuous, diffuse pain in the heel region, without particular predominance of pain in the morning hours is mentioned. On US, calcaneal spur is seen in a view of hyperechoic lesion of varying size in continuity with calcaneal bone which may be covered by a thick hypoechoic structure that corresponds to the enlarged plantar aponeurosis. In a particular patient, its thickness is 4.2mm (3-4mm is considered as a normal range), (figure 10a).
{kind=link}
On the contrary, if patients complains for pain that is clearly limited over the area of the medial heel and with inability to support in the morning hours the US image shows a hyperechoic spur which is overlaid by an enlarged hypoechoic structure that corresponds to the plantar aponeurosis. Its thickness in this typical case of plantar fasciitis reaches 6 mm in the middle of the lesion (compared to 3-4mm), (figure 10b).
{kind=link}
When persistent pain is located distally to the heel, a fusiform, homogeneously hypoechoic mass is sometimes detected in the region of the medial third of the plantar aponeurosis, known as plantar fibromatosis – Ledderhose disease, (figure 11).
{kind=link}
Bibliography:
- Bruyn GAW , Schmidt WA. Introductory Guide to Musculoskeletal Ultrasound for the Rheumatologist, Bon Stafleu van Loghum, the Netherlands, 2006.
- Bianchi S, Martinoli C. Ultrasound of the Musculoskeletal System, Springer-Verlag, Berlin, 2007.
- Backhaus M, Burmester G-R, Gerber T et al. Guidelines for Musculoskeletal Ultrasound in Rheumatology. Ann Rheum Dis 2001;60:641-649.
- Wakefield J.R, D’Agostino MA. Essential applications of Musculoskeletal Ultrasound in Rheumatology, Saunders Elsevier, Philadelphia,
- Holsbeeck T.M, Introcaso H.J. Musculoskeletal Ultrasound, Mosby of Elsevier, St Louis, Missouri, 2001.
- Filipucci E, Iagnocco A, Meenagh G et al. Ultrasound Imaging for the Rheumatologist. VII.Ultrasound Imaging in Rheumatoid Artrhritis. Clin Exp Rheum 2007;25:5-10.
- Balint PV, Kane D, Wilson H, McInnes IB, Sturrock RD. Ultrasonography of entheseal insertions in the lower limb in spondyloarthropathy. Ann Rheum Dis 2002;61:905–10.
- D’Agostino MA, Said-Nahal R, Hacquard-Bouder C, Brasseur JL, Dougados M, Breban M. Assessment of peripheral enthesitis in the spondylarthropathies by ultrasonography combined with power Doppler: a cross-sectional study. Arthritis Rheum 2003;48:523–33.
- McGonagle D, Marzo-Ortega H, O’Connor P et al. Histological assessment of the early enthesitis lesion in spondyloarthropathy. Ann Rheum Dis 2002;61:534–7.
- Nazarian LN, Rawool NM, Martin CE, Schweitzer ME. Synovial fluid in the hindfoot and ankle: detection of amount and distribution with US. Radiology 1995;197:275–8.
- Filer A, de Pablo P, Allen G et al. Utility of ultrasound joint counts in patients with very early synovitis. Ann Rheum Dis 2011;70(3):500-7
- Backhaus M. Ultrasound and structural changes in inflammatory arthritis – synovitis and tenosynovitis. Ann N Y Acad Sci. 2009 Feb;1154:139-51. Review.
- Martinoli C, Bianchi S, Derchi LE. Tendon and nerve sonography. Radiol Clin North Am 1999;37:691–711, viii.
- Grassi W, Meenagh G,. Pascual E, Filippucci E. “Crystal Clear”—Sonographic Assessment of Gout and Calcium Pyrophosphate Deposition Disease. Semin Arthritis Rheum 2006;36:197-202
- Frediani B, Filippou G, Falsetti P, Lorenzini S, Baldi F, Acciai C, et al. Diagnosis of calcium pyrophosphate dihydrate crystal deposition disease: ultrasonographic criteria proposed. Ann Rheum Dis 2005;64:638-40.
- Meenagh G, Filippucci E, Delle Sedie et al. Ultrasound imaging for the rheumatologist. XVIII. Ultrasound measurements. Clin Exp Rheumatol. 2008 Nov-Dec;26(6):982-5.
- Rosenberg C, Etchepare F, Fautrel Bet al. Diagnosis of synovitis by ultrasonography in RA: a one-year experience is enough for reliability on static images. Joint Bone Spine. 2009 Jan;76(1):35-8.